Rethinking Concussion Recovery: The Case for Active Rehabilitation Concussions are more than just a bump on the head, or “getting your bell rung”; they are a type of mild traumatic…
Introduction Appropriate concussion management is crucial for ensuring the well-being and long-term health of individuals who have experienced a mild traumatic brain injury. One aspect of concussion management that has…
How Hard is Too Hard? Examining the Forces Behind Concussive Impacts.
Introduction to Concussions A concussion (or mild traumatic brain injury) is a type of traumatic brain injury (TBI) that occurs when the brain experiences sudden movement or impact. This can…
Every suspected traumatic brain injury warrants a thorough neurological examination. As you conduct your exam, it is important to remember that a brain injury may include structural or functional compromise…
Historically, healthcare providers told patients with concussion symptoms due to mild traumatic brain injury to rest, rest, rest. And, when complete rest didn’t work, healthcare providers told them to rest some more.
The research on concussions and post-concussion syndrome is evolving at an exponential rate, and we realize that not only does prolonged mental rest not work, but it can also make your post-concussion symptoms worse.
Sadly, many healthcare providers are not keeping up with the explosion in post-concussion syndrome research and are still not up to speed on how to treat a concussion. They continue telling their patients that the only treatment for a head injury is mental rest. If you have fallen victim to this, you don’t need more rest; you need a second opinion.
While relative rest is still important during the early stages following injury, that timeline is getting shorter (i.e., 48 hours of relative rest), with strict, prolonged rest starting to worsen patient symptoms over time. So, although you may have been told to rest at the emergency room, if it’s been more than ten days of symptoms, it’s time to switch it up and start finding better concussion-supportive therapy before your symptoms worsen. (1)
If not rest, then what?
The Top 5 Most Effective Evidence-Based Treatment Options for Concussion & Post-Concussion Syndrome:
In this article, we are exploring the best concussion therapies to treat your mild traumatic brain injury – especially those suffering from persistent symptoms. Concussion recovery involves more than just treating the brain – a good concussion specialist will look at all the reasons why persistent concussion symptoms occur and take into account your previous concussion history, your physical & cognitive symptoms, your vestibular system, mood changes, and mental health disorders, and implement a concussion treatment plan that should include the following elements as part of their post-concussion treatment 5 step program:
Exercise Therapy
Manual Therapy & Neck Injury Rehab
Diet & Nutritional Changes
Vision Therapy & Vestibular Therapy
Education
Let’s explore why each one of these areas is so vital to concussion recovery and helping symptoms resolve for patients suffering from post-concussion syndrome.
If you’d rather watch, here is a video explaining the Top Concussion Treatments from an Episode of Ask Concussion Doc
1. Exercise Therapy
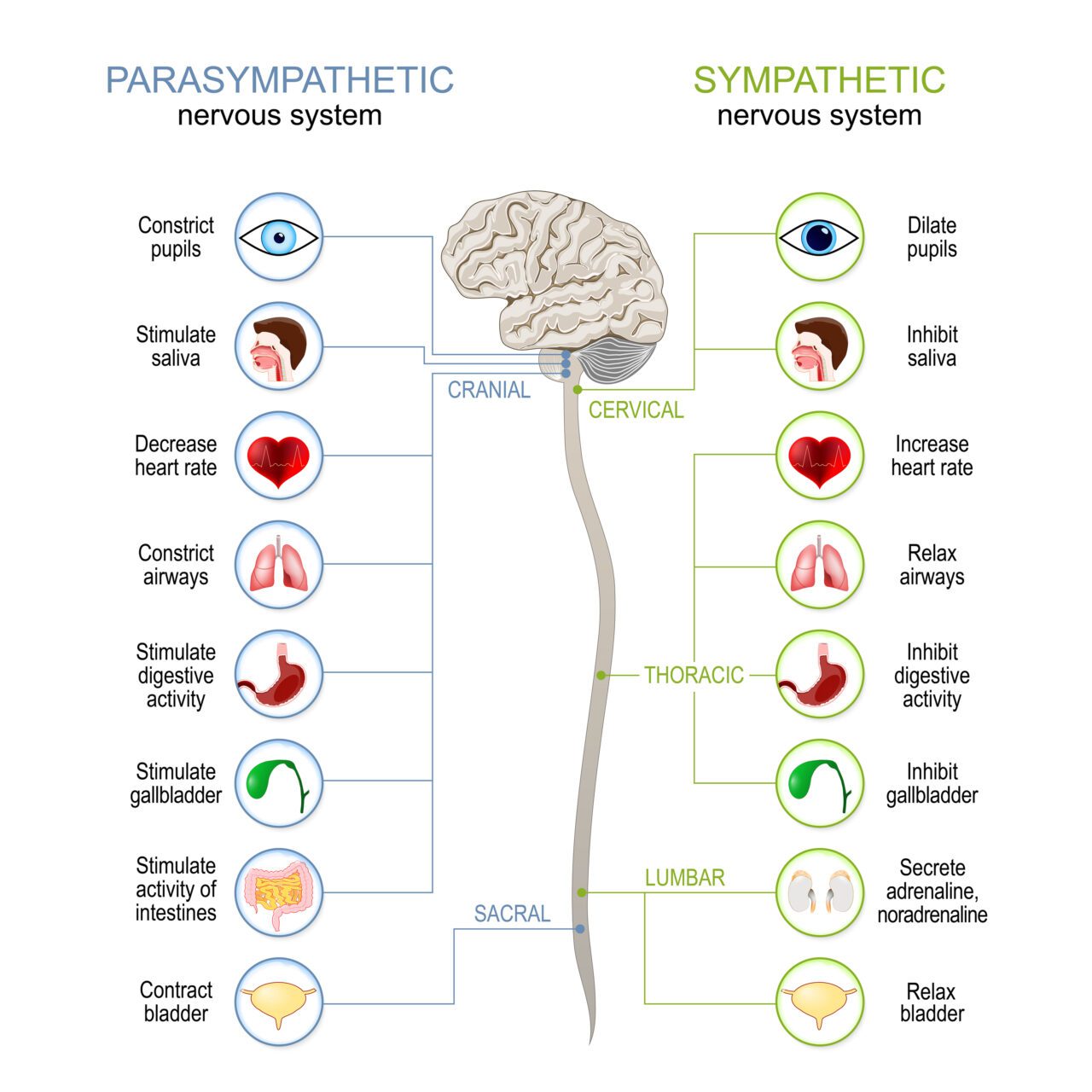
Following a traumatic brain injury, animal (and many human) studies have demonstrated an alteration in blood flow to the brain. (2) Recent post-concussion research has found that these blood flow changes may persist for some time following injury due to ongoing dysfunction in the Autonomic Nervous System (ANS). (3,4,5,6)The ANS consists of two differing sides: the sympathetic nervous system and the parasympathetic nervous system.
Sympathetic And Parasympathetic Nervous System
The Sympathetic Nervous System (SNS)
The SNS is also known as the “Fight, Flight, or Freeze” system. This side of the ANS is responsible for increasing our heart rate, dilating our blood vessels to pump blood to our muscles, releasing adrenaline, dilating our pupils, and preparing for action.
The Parasympathetic Nervous System (PNS)
The PNS, on the other hand, is our “Rest & Digest” system. This side of the ANS is responsible for lowering our heart rate, increasing our saliva production and digestion, activating our metabolism, and helping us feel relaxed and calm.
These two systems can be thought of as a teeter-totter. When one is up, the other is down—but not necessarily “on vs. off.” They fluctuate in relative dominance throughout our days and play synergistic roles in our individual actions (e.g., micturition or “peeing” requires both SNS and PNS activity). Overall, our autonomic nervous system works to maintain harmony and balance.
Brain injury creates an imbalance in the ANS, with most suffering from a shift toward a high “sympathetic tone” – this means that we get stuck in a bias toward a “fight or flight” state. Our heart rate tends to be more elevated than usual and doesn’t respond well to increased demands; blood flow to our brain is not as well-regulated; our digestion may slow down, leading to stomach pains, food sensitivities, and increased inflammation; our anxiety levels rise, we may get lightheaded more easily, and we may suffer symptoms with slight increases in everyday activities.
The good news is that research is improving at testing for and treating this problem very quickly, provided you know what you’re doing!
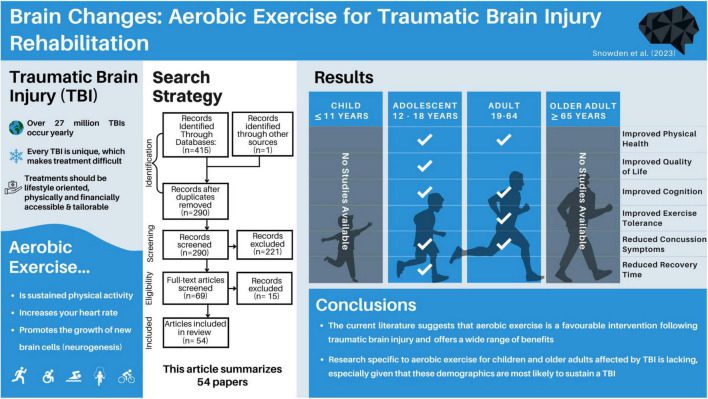
The solution for this problem goes against conventional thought: exercise! (7)
Image from PMID: 38188504
Pioneered by the University of Buffalo researchers, numerous studies have demonstrated complete resolution of signs and symptoms and improved brain blood flow (as measured on fMRI) through a specific graded exercise program alone. (8)
More recent evidence suggests that exercise helps speed recovery after a concussion—as early as within the same week of the injury! (1)
This type of testing and exercise prescription is usually carried out by a physical therapist, occupational therapists, athletic trainers, or chiropractors. It is essential to see a healthcare provider who knows exactly what they are doing with this protocol and has received advanced training in the treatment of head injury and post-concussion syndrome. Testing with a trained healthcare provider must be done first to establish set points and your specific program.
2. Manual Therapy & Neck Rehab
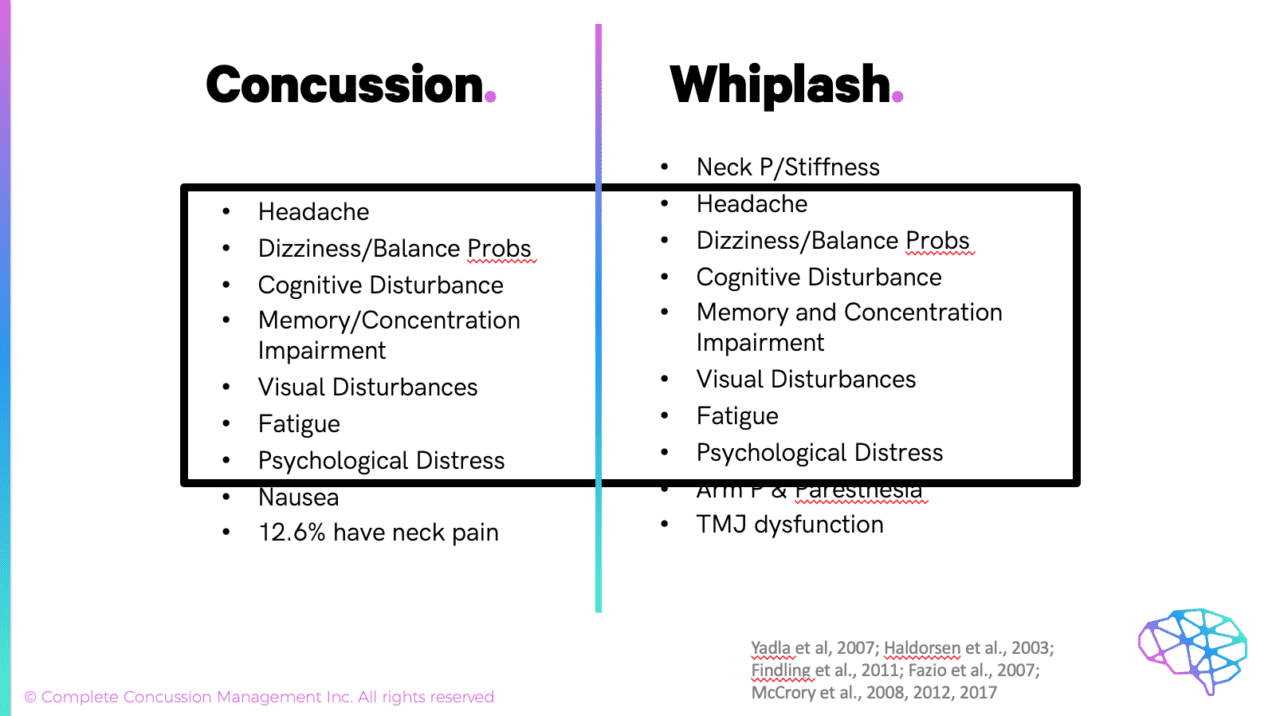
With every concussion, there is also a whiplash element of the initial injury.
Studies have demonstrated that the acceleration required to cause a concussion is between 70 and 120 G’s (where G = force of gravity = 9.8m/s2). Whiplash, on the other hand, has been shown to occur at only 4.5 G’s. (9,10,11)
It is, therefore, conceivably impossible for a concussion to occur without also causing a sprain or strain injury to your neck! This is a repeatable finding in the research; these injuries are happening together. (12,13)
What becomes even more confusing is that the signs and symptoms of whiplash and neck dysfunction are the same as concussion symptoms! Headaches, problems with cognitive tasks, emotional issues & mood swings, balance problems and dizziness, eye movement control problems, and brain blood flow abnormalities have all been shown to occur in post-concussive syndrome as well as whiplash and neck pain patients.(14,15,16,17)
Unfortunately, there is no way to tell if the symptoms are coming from your neck or your concussion except with testing (some specific tests that we won’t go into here). Most of the head injury patients in this category don’t even report any neck pain, which makes this all the more confusing for the average medical provider.
So, if you are still having post-concussion symptoms, even if you don’t have neck pain, you may be suffering from symptoms that are coming from your neck, which are easily treated with physical therapy consisting of manual therapy and rehabilitative exercises.
3. Diet/Nutritional Changes
During the recovery process following an injury to any tissue, there is inflammation; post-concussion patients are no exception, with several studies demonstrating increased inflammatory markers following brain injury. (18,19)
Concussion results in metabolic dysfunction (read: energy deficit) in the initial stages, which is why strict rest used to be prescribed as part of the immediate medical care to help the brain recover. The thought was – anything that burns energy, such as thinking or physical activity, could worsen symptoms. As mentioned above, however, rest is no longer considered an effective post-concussion treatment.
The majority of studies examining this metabolic disruption show a recovery between 22 and 45 days after injury. (20,21) In other words, beyond a 3-6 week period, there is little metabolic explanation for your symptoms, provided you didn’t suffer a second concussion during that time window.
Treatment options for both metabolic dysfunction and neuro-inflammation include simple dietary changes such as avoiding pro-inflammatory foods (refined sugars, white bread, pasta, artificial sweeteners, etc) and replacing them with healthier options such as fruits and vegetables, freshly caught fish (salmon, mackerel, herring), and good fats (coconut oil, flax seed, almonds). These changes may offset an ongoing inflammatory response and reduce your concussion symptoms. (22)
Although still in its infancy, there is increasing support for various supplements such as Omega-3 fatty acids, creatine, curcumin, magnesium glycinate, and melatonin. (23,24,25,26,27,28,29,30,31)Please speak with your concussion specialist before starting on any supplements, as there can occasionally be adverse effects and/or interactions with other medications that you may be taking.
Another option would be to speak to your doctor about a short course of anti-inflammatory medications. Note that we say “short course” as, over a prolonged period, these medications are not an effective treatment option.
4. Vestibular and Visual Rehab
Dizziness and balance problems are some of the most common ongoing concussion symptoms associated with post-concussion syndrome. This may be due to several overlapping issues such as problems with the balance centers of your brain (vestibular system), your visual system, and/or problems with the muscle and joint sensors of your neck. (17)
Problems with the visual system may also be one of the causes of ongoing cognitive complaints such as trouble with concentration and/or memory. If you find yourself reading a passage and then having to re-read it several times before you understand what it is saying, you might have a problem with how your eyes are moving or working together. If so, this may require vision therapy (also known as neuro-optometric rehabilitation) as opposed to occupational therapy or cognitive therapy.
These categories are placed together because it is often difficult to tell where persistent symptoms of dizziness and visual issues are coming from. Sometimes, these issues require physical therapy or chiropractic care (mostly vestibular therapy and manual therapy/rehabilitation of the neck), and sometimes, you require neuro-optometric rehabilitation or vision therapy from a neuro-optometrist.
Testing for each of these areas requires extensive knowledge of each of the systems and how they may interact. If you have not had extensive testing of these systems as part of your head injury care, then you are in the wrong place!
A proper rehabilitation program can be set up following a thorough assessment of these areas and a thorough neurological examination. The research on rehabilitation for these areas is extensive with numerous studies showing the resolution of dizziness and visual abnormalities, with a fairly short course of treatment. (32,33)
5. Education and Reassurance (due to Psychological Comorbidities)
It has been well established that patients with a pre-existing history of depression and/or anxiety tend to have an increased risk of post-concussion syndrome.(34,35) Not only that, the symptoms of these and other mental health conditions can result in, or mimic, the same symptoms of concussion (dizziness, mental confusion, concentration problems, sadness, emotional outbursts, and mood swings). (36,37,38) Many of these issues can begin before or after the head injury, which may be due to the brain injury itself, or a direct result of being mismanaged by an uninformed healthcare provider. (39,40) In other words, being told to sit in a dark room, avoid all social contact, not go to work or school, and not do any physical activity for months on end may be causing the very anxiety, depression, and triggering symptoms that you are attempting to eliminate.
Studies examining the overlay of mental health conditions and post-concussion symptoms are endless (so much so that I won’t even begin to start referencing them), and mental health will always be a big part of concussion management. In many cases, patients often feel much better just learning about their condition and learning that it is 100% treatable, given the right approach. The Ontario Neurotrauma Foundation recently demonstrated that one of the best evidence-based treatment options for preventing long-term symptoms was patient education and reassurance! (41) Just by helping the patient to be better informed about their condition and the effective treatment options available for post-concussion syndrome allows concussion patients to be empowered to seek out effective post-concussion treatment.
Hopefully, reading this article has made you feel better about your condition. In more serious cases, you may need to see a psychologist, psychiatrist, or other mental health professional such as a social worker. If you feel that you are depressed or hopeless, please talk to your doctor or seek the help of a mental health professional!
There is help out there! The trick is finding the right clinic, practitioner, or team that can help you. Click here for our interactive map to find a concussion specialist clinic near you!
What to Do For a Concussion at Home
If you are reading this blog and realize that you have not been able to find a good concussion clinic close to where you live, there are other options that you may find helpful. One such amazing resource that we have found is the Concussion Fix program.
The Concussion Fix Program is an online concussion treatment program designed to help patients with persistent symptoms figure out what is driving their symptoms and how to fix them. The program is based on the latest scientific research and is tailored to the individual needs of each patient. The program teaches patients how to balance the autonomic nervous system, how to improve their diet to fix metabolic and neuro-inflammatory issues, and how to safely return to work and life.
The Concussion Fix Program has helped thousands of patients worldwide get back to living their lives without the debilitating symptoms of post-concussion syndrome. If you can’t find a good clinic near you, the Concussion Fix is an extremely inexpensive and effective program for reducing your post-concussive symptoms.
Patricios JS, Schneider KJ, Dvorak J, et al. Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport–Amsterdam, October 2022, British Journal of Sports Medicine 2023;57:695-711.
Len TK, Neary JP. Cerebrovascular pathophysiology following mild traumatic brain injury, March 2011, Clin Physiol Funct Imaging;31(2):85-93. doi: 10.1111/j.1475-097X.2010.00990.
Meier TB, Bellgowan PSF, Singh R, Kuplicki R, Polanski DW, Mayer AR. Recovery of cerebral blood flow following sports-related concussion, May 2015, JAMA Neurol;72(5):530-8. doi: 10.1001/jamaneurol.2014.4778.
Wang Y, Nelson LD, LaRoche AA, Pfaller AY, Nencka AS, Koch KM, McCrea MA. Cerebral Blood Flow Alterations in Acute Sport-Related Concussion, Jul 2016, J Neurotrauma;33(13): 1227-36. doi: 10.1089/neu.2015.4072.
Wang Y, Nencka AS, Meier TB, Guskiewicz K, Mihalik JP, et.al. Cerebral blood flow in acute concussion: preliminary ASL findings from the NCAA-DoD CARE consortium, Oct 2019, Brain Imaging Behav;13(5): 1375-1385. doi: 10.1007/s11682-018-9946-5.
Callaway CCM, Kosofsky, BE. Autonomic dysfunction following mild traumatic brain injury, Dec 2019, Curr Opin Neurol;32(6):802-807. doi: 10.1097/WCO.0000000000000751.
Snowden T, Morrison J, Boerstra M, Eyolfson E, Acosta C, et.al. Brain changes: aerobic exercise for traumatic brain injury rehabilitation, Dec 2023, Front Hum Neurosci.;17: 1307507. doi: 10.3389/fnhum.2023.1307507
Leddy JJ, Burma JS, Toomey CM, Hayden A, Davis GA, et.al. Rest and exercise early after sport-related concussion: a systematic review and meta-analysis, June 2023, Br J Sports Med;57(12):762-770. doi: 10.1136/bjsports-2022-106676.
Viano DC, Casson IR, Pellman EJ. Concussion in professional football: biomechanics of the struck player–part 14, Aug 2007, Neurosurgery; 61(2):313-27. doi: 10.1227/01.NEU.0000279969.02685.D0.
Viano DC, &Pellman EJ. Concussion in professional football: biomechanics of the striking player–part 8, Feb 2005, Neurosurgery; 56(2):266-80. doi: 10.1227/01.neu.0000150035.54230.3c.
Slade, S. (2009). Feel the G’s: The Science of Gravity and G-forces. Capstone.
Marshall CM, Vernon H, Leddy JJ, Baldwin BA. The role of the cervical spine in post-concussion syndrome, Jul 2015, Phys Sportsmed.; 43(3):274-84. doi: 10.1080/00913847.2015.1064301.
Hynes LM, & Dickey JP. Is there a relationship between whiplash associated disorders and concussion in hockey? A preliminary study, Feb 2006, Brain Inj.; 20(2):179-88. doi: 10.1080/02699050500443707.
Yadla S, Ratliff JK, Harrop JS, Whiplash: diagnosis, treatment and associated injuries, Mar 2008, Curr Rev Musculoskelet Med.;1(1):65-8.doi: 10.1007/s12178-007-9008-x.
Haldorsen T, Waterloo K, Dahl A, Mellgren SI, Davidsen PE, Molin PK, Symptoms and cognitive dysfunction in patients with the late whiplash syndrome, 2003, Appl Neuropsychol.;10(3):170-5. doi: 10.1207/S15324826AN1003_06.
Findling O, Schuster C, Sellner J, Ettlin T, Allum JHJ, Trunk sway in patients with and without, mild traumatic brain injury after whiplash injury, Oct 2011, Gait Posture.;34(4):473-8.doi: 10.1016/j.gaitpost.2011.06.021.
Cheever K, Kawata K, Tierney R, Galgon A. Cervical injury assessments for concussion evaluation: a review, Dec 2016, J Athl Train.;51(12):1037-1044.doi: 10.4085/1062-6050-51.12.15.
Visser K, Koggel M, Blaauw J,van der Horn HJ, Jacobs B, et.al. Blood-based biomarkers of inflammation in mild traumatic brain injury: A systematic review, Jan 2022, Neurosci Biobehav Rev.;132:154-168.doi: 10.1016/j.neubiorev.2021.11.036.
Neumann KD,Broshek DK, Newman BT, Druzgal TJ, Kundu BK, Resch JE. Concussion: Beyond the Cascade, Aug 2023, Cells.;2(17):2128.doi: 10.3390/cells12172128.
Vagnozzi R, Tavazzi B, Signoretti S, Amorini AM, Belli A et.al. Temporal window of metabolic vulnerability to concussions: mitochondrial-related impairment–part I, Aug 2007, Neurosurgery.;61(2):379-88; discussion 388-9. doi: 10.1227/01.NEU.0000280002.41696.D8.
Signoretti S, Lazzarino G, Tavazzi B, Vagnozzi R. The pathophysiology of concussion, Oct 2011, PM R.;3(10 Suppl 2):S359-68.doi: 10.1016/j.pmrj.2011.07.018.
Shaito A, Hasan H, Habashy KJ,Fakih W, Abdelhady S, et.al. Western diet aggravates neuronal insult in post-traumatic brain injury: Proposed pathways for interplay, Jul 2020, EBioMedicine.;57:102829.doi: 10.1016/j.ebiom.2020.102829.Epub 2020 Jun 20.
Ashbaugh A, McGrew C. The role of nutritional supplements in sports concussion treatment, Jan-Feb 2016, Curr Sports Med Rep.;15(1):16-9. doi: 10.1249/JSR.0000000000000219.
Trojian TH, Wang DH, Leddy JJ. Nutritional supplements for the treatment and prevention of sports-related concussion-evidence still lacking, Jul/Aug 2017, Curr Sports Med Rep.;16(4):247-255.doi: 10.1249/JSR.0000000000000387.
Kreider RB, Kalman DS, Antonio J, Ziegenfuss TN, Wildman R et.al. International Society of Sports Nutrition Position Stand: safety and efficacy of creatine supplementation in exercise, sport and medicine, Jun 2017, J Int Soc Sports Nutr.;13:14:18. doi: 10.1186/s12970-017-0173-z.
Roschel H, Gualano B, Ostojic SM, Rawson ES. Creatine supplementation and brain health, Feb 2021, Nutrients.;10;13(2):586.doi: 10.3390/nu13020586.
Mishra S, Singh VJ, Chawla PA, Chawla V. Neuroprotective role of nutritional supplementation in athletes, 2022, Curr Mol Pharmacol.;15(1):129-142.doi: 10.2174/1874467214666211209144721.
Oliver JM, Anzalone AJ, Turner SM. Protection before impact: the potential neuroprotective role of nutritional supplementation in sports-related head trauma, Mar 2018, Sports Med.;48(Suppl 1):39-52.doi: 10.1007/s40279-017-0847-3.
Petraglia AL, Winkler EA, Bailes JE. Stuck at the bench: Potential neuroprotective compounds for concussion, 2011, Surg Neurol Int.;2:146.doi: 10.4103/2152-7806.85987.
Finnegan E, Daly E, Pearce AJ, Ryan L. Nutritional interventions to support acute mTBI recovery, Oct 2022, Front Nutr.;14:9:977728.doi: 10.3389/fnut.2022.977728.
Ryan T, Nagle S, Daly E, Pearce AJ, Ryan L. A potential role exists for nutritional interventions in the chronic phase of mild traumatic brain injury, concussion and sport-related concussion: A systematic review, Aug 2023, Nutrients.;15(17):3726. doi: 10.3390/nu15173726.
Babula G, Warunek E, Cure K, Nikolski G, Fritz H, Barker S. Vestibular rehabilitation as an early intervention in athletes who are post-concussion: a systematic review, Jun 2023, Int J Sports Phys Ther.;1;V18(3):577-586.doi: 10.26603/001c.75369.
Art K, Ridenour C, Durbin S, Bauer M, Amy Hassen-Miller A. The effectiveness of physical therapy interventions for athletes post-concussion: a systematic review, Feb 2023, Int J Sports Phys Ther.;1;18(1):26-38.doi: 10.26603/001c.68071.
Broshek DK, De Marco AP, Freeman JR. A review of post-concussion syndrome and psychological factors associated with concussion, 2015, Brain Inj.;29(2):228-37. doi: 10.3109/02699052.2014.974674.
Cuff S, Maki A, Feiss R, Young J, Shi J, et.al. Risks factors for prolonged recovery from concussion in young patients, Dec 2022, Br J Sports Med.;56(23):1345-1352.doi: 10.1136/bjsports-2022-105598.
Hilber P. The role of the cerebellar and vestibular networks in anxiety disorder and depression: the internal model hypothesis, Oct 2022, Cerebellum.;21(5):791-800.doi: 10.1007/s12311-022-01400-9.
Hilber P, Cendelin J, Le Gall A, Machado M, Tuma J, et.al. Cooperation of the vestibular and cerebellar networks in anxiety disorders and depression, Mar 2019, Prog Neuropsychopharmacol Biol Psychiatry.;8:89:310-321. doi: 10.1016/j.pnpbp.2018.10.004.
Maywald M, Pogarell O, Levai S, Paolini M, Tschentscher N, et.al. Neurofunctional differences and similarities between persistent postural-perceptual dizziness in anxiety disorder, 2023, Neuroimage Clin.;37:103330. doi: 10.1016/j.nicl.2023.103330.
Kirkwood MW, Howell DR, Brooks BL, Wilson JC, Meehan Iii WP. The nocebo effect and pediatric concussion, May 2021, J Sport Rehabil.;30(6):837-843. doi: 10.1123/jsr.2020-0519.
Polich G, Iaccarino MA, Kaptchuk TJ, Morales-Quezada L, Zafonte R. Nocebo effects in concussion:is all that is told beneficial?, Jan 2020, Am J Phys Med Rehabil.;99(1):71-80. doi: 10.1097/PHM.0000000000001290.
Complete Concussions specializes in collaborative, evidence-based concussion care. Our evidence-based training programs and integrated healthcare technologies empower multidisciplinary teams to implement standardized care for those impacted by concussions.
Our network and patient database enables large-scale research to advance concussion management, and ultimately, the long-term health and well-being of concussion patients and also teach them some concussion care at home.
We analyze leading research to develop best-in-class approaches to concussion care.