What Flavor/Subtype of Concussion Does Your Patient Have? Psychological Type Deep-dive
Which of the Concussion Subtypes are Driving Your Patient’s Symptoms? A Psychological Type Deep-dive Welcome to the last and final part of the deep dive into the 4 different mild…
What Flavor/Subtype of Concussion Does Your Patient Have? Cervical Spine (Vestibulospinal) Type Deep-Dive
The majority of individuals, approximately 60-70%, who sustain a concussion will recover within 4 weeks. While many strive to be among this majority, about 30-40% of concussion patients will experience…
What Flavor/Subtype of Concussion Does Your Patient Have? Visual/Vestibular (Vestibuloocular) Type Deep-Dive
Introduction Post Concussion Syndrome (PCS) is a complex disorder in which various common concussion symptoms — such as headaches, dizziness, and cognitive dysfunction — persist for weeks, months, or even…
Concussions are often called invisible injuries, leaving patients with a myriad of physical, cognitive, and emotional symptoms. One unifying driver between all these symptoms can be a deceptively simple problem: blood flow. This brings us to our deep dive into the autonomic nervous system (ANS) as it relates to concussion symptoms and rehab. By the end, you will be able to identify the patients that fit into this subtype, know how to assess them and know the main features of evidence-based rehabilitation or referral.
The “Autonomic/Physiologic Patient”.
Let’s say that Jake from State Farm walks into your office. His main complaint is a migraine-like headache that seems to be made worse by everything: loud cars on the street, reading work emails, walking up the stairs to his apartment, etc. The big problem is that Jake needs to be present for work meetings where multiple people will be talking, and he needs to be cognitively ready to respond to questions and make business decisions. Jake also wonders when he’ll ever be able to tolerate getting back on his road bike.
Jake sounds like your average concussion patient – more specifically, Jake sounds like a patient with autonomic (blood flow) issues.
The key features of your autonomic patient will be:
Hypersensitivity to various stimuli (e.g., lights, sounds, visual motion, etc.)
Transient visual/vestibular symptoms
The main triggers for autonomic/physiologic patients are:
Sustained cognitive or physical activity
Increasing intensity/duration of activity
Why do we Think This Happens?
The known pathophysiology of concussion involves a neurometabolic cascade secondary to widespread functional stretching and shearing of neurons. Following this, there are three proposed mechanisms for how a concussion disrupts autonomic function:
Possible sub-radiographic axonal injury, secondary to the stretching and shearing.
Possible cortical spreading depression (similar to migraine) secondary to the excitotoxicity seen in the neurometabolic cascade.
Global cerebral metabolic disturbances involving the ANS that result in disrupted cerebral blood flow.
Now, it’s this third proposed mechanism, altered brain blood flow, with the most significant research behind it.
The brain regulates blood flow by:
Monitoring CO2 levels (cerebrovascular reactivity)
Supporting active brain tissue (neurovascular coupling).
Multiple studies show that each of these mechanisms can be disrupted following a concussion, resulting in both too much and too little blood flow at inappropriate times – leading to an increase in your patient’s symptoms (e.g., head pressure, fogginess, dizziness, nausea, etc.).
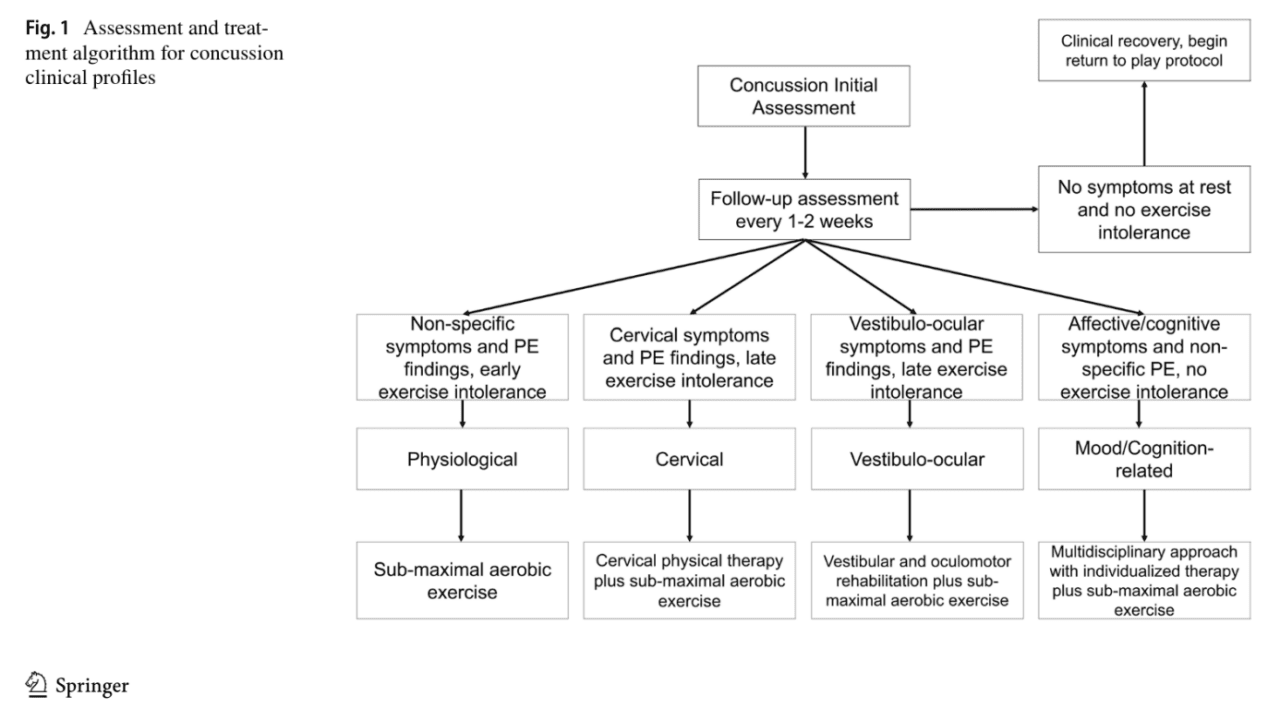
Next Steps: How do we Assess and Confirm Autonomic Issues?
We must systematically assess for autonomic dysfunction in nearly all patients presenting with concussion/PCS, as this can be the missing link in many patients who were told to “rest until symptoms go away” and in patients who may have an underlying or triggered dysautonomia (e.g., POTS).
Neurologists and concussion specialists are urged to assess autonomic function in two very accessible ways:
Orthostatic Vital Signs (e.g., Active or Modified Active Standing Test)
Buffalo Concussion Treadmill/Bike Test (e.g., BCTT or BCBT)
It is recommended that you also assess in that order: Orthostatic → Exercise Tolerance. Intuitively, patients who cannot tolerate gravity (e.g., orthostatic intolerance) will certainly not tolerate exercise (e.g., BCTT).
1. Orthostatic Vital signs
This is a fancy name for a simple assessment: “How well does my patient adjust their heart rate and blood pressure from supine to standing (i.e., gravity)?” The proposed gold standard for this testing is the Head-Up Tilt Table Test, though the Active Standing Test is proving to be comparable and more accessible (https://pubmed.ncbi.nlm.nih.gov/23731914/)
3 Ways to Test:
2min OH Screen: Measure vitals after supine for 2min, and again after standing for 1min.
Active Standing Test:Measure vitals after 5min supine and at 2, 5, 7, and 10min standing.
Modified Active Standing Test (https://pubmed.ncbi.nlm.nih.gov/35647216/): Measure vitals after each condition: Supine for 2min, seated for 2min, and standing for 2min.
Normally, a patient’s blood pressure should not change appreciably, and heart rate should only increase 10-30 bpm in adults (10-40bpm in children).
Interpreting Orthostatic Vitals:
With these vitals, we are screening for three main conditions: Orthostatic Tachycardia (e.g., POTS), Orthostatic Hypotension, and Hypovolemia.
Condition
20yo and older
19yo and younger
Orthostatic Tachycardia
Heart rate between supine and standing positions increases by more than 30 BPM (or standing heart rate is greater than 120 BPM) and systolic blood pressure has not decreased by 20 mmHg or diastolic blood pressure has not decreased by 10 mmHg.
Heart rate between supine and standing positions increases by more than 40 BPM (or standing heart rate is greater than 120 BPM) and systolic blood pressure has not decreased by 20 mmHg or diastolic blood pressure has not decreased by 10 mmHg.
OrthostaticHypotension
Heart rate between supine and standing positions has not increased by 30 BPM and systolic blood pressure has decreased by 20 mmHg or diastolic blood pressure has decreased by 10 mmHg.
Heart rate between supine and standing positions has not increased by 40 BPM and systolic blood pressure has decreased by 20 mmHg or diastolic blood pressure has decreased by 10 mmHg.
Hypovolemia
Heart rate between supine and standing positions has increased by 30 BPM (or standing heart rate is greater than 120 BPM) and systolic blood pressure has decreased by 20 mmHg or diastolic blood pressure has decreased by 10 mmHg.
Heart rate between supine and standing positions has increased by 40 BPM (or standing heart rate is greater than 120 BPM) and systolic blood pressure has decreased by 20 mmHg or diastolic blood pressure has decreased by 10 mmHg.
2. Buffalo Concussion Treadmill Test (BCTT)
This is a submaximal (i.e., walking) test based on a Balke Protocol used to assess VO2max. Dr. John Leddy and his team have worked to make this one of the most useful and valid tools in assessing and managing concussion/PCS.
In the autonomic/physiologic patient, we typically observe “early exercise intolerance” when performing the BCTT. These patients typically have symptom(s) flare when intensities reach 50-70% of their estimated HRmax – classically considered light to moderate intensity zones.
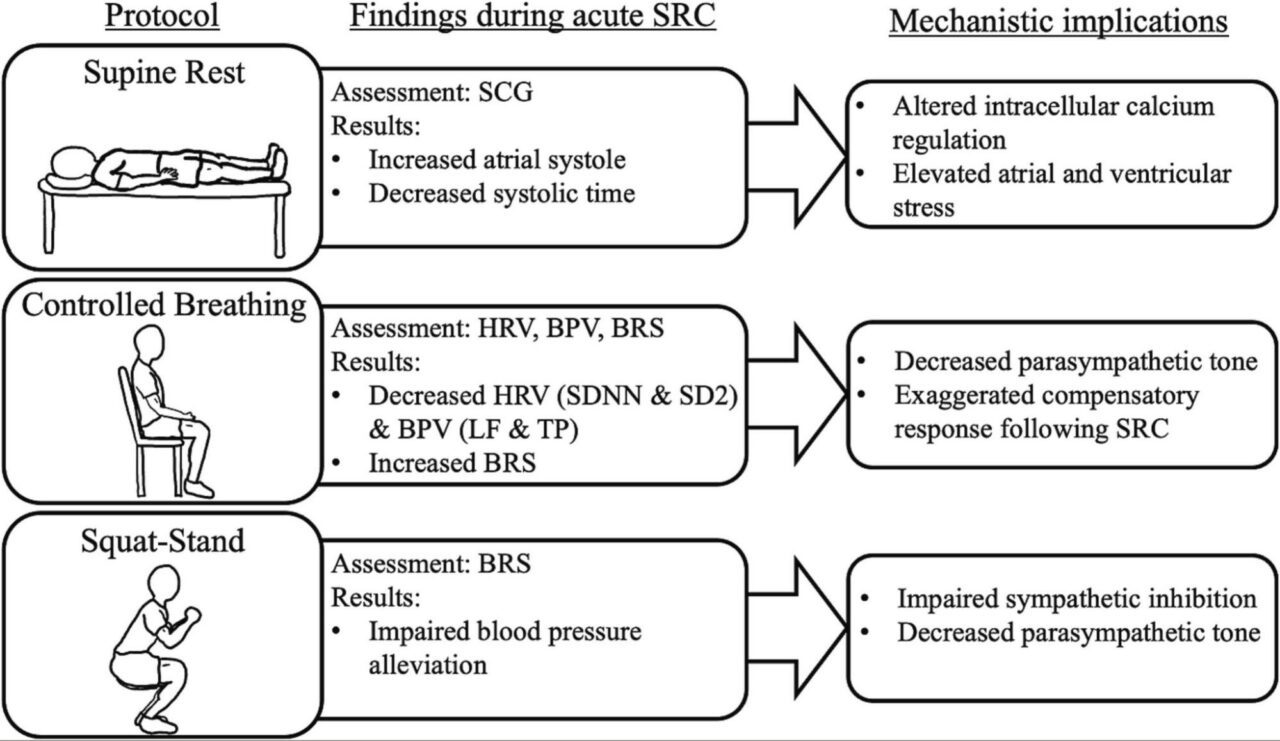
Most recently, a 2024 paper reviewed autonomic assessments and pinned down four variables that may be the easiest to study and put into clinical practice moving forward. They measured Heart rate variability (HRV), Blood pressure variability (BRV), Baroreflex sensitivity (BRS), and altered cardiac cycle timing and contractility in the context of a “Supine, Seated, Squatting” Test.
However, the most practical and accessible assessments today are still orthostatic vitals and submaximal exercise testing.
How do we Treat Autonomic Dysfunction?
This is where the road becomes extremely simple – or tricky.
Exercise is Medicine.
The best, evidence-based approach to date is to start with sub-symptom aerobic exercise based on your patient’s BCTT results. This is the most common and successful approach across the majority of patients with concussion or PCS – regardless of the main concussion subtype.
In the case of POTS or borderline orthostatic tachycardia, we can consider implementing the Levine or CHOP protocols. However, these cases can become more complex and often require an interdisciplinary care team.
Breathe… slowly.
An approach that works like “peanut butter and jelly” (at least in the USA) is pairing your patient’s sub-symptom aerobic exercise protocol with slow nasal breathing. Taking the breathing rate below 10 breaths per minute is now “clinically slow.” The range that evokes the highest HRV and coherence (good things) is between 4.5 and 6.5 breaths per minute (bpm), with an average settling on 6bpm. A couple of examples of popular and effective 6bpm breathing strategies are below:
5:5 Breathing: Inhale for 5 seconds, exhale for 5 seconds.
4:6 Breathing: Inhale for 4 seconds, exhale for 6 seconds.
Address co-existing conditions or symptoms.
Altered autonomic function is not limited to heart rate or blood pressure abnormalities. For example, postural orthostatic tachycardia (POTS) can present with both cardiac symptoms (e.g., tachycardia, presyncope, dyspnea, etc.) and non-cardiac symptoms (e.g., abdominal pain, bloating, diarrhea, etc.). These “extra” symptoms are in-part blood flow-related but may also be related to dysregulated immune function (e.g., mast cell activation).
We also know a strong relationship exists between vestibular function and cardiovascular/autonomic function (i.e., vestibulosympathetic reflex). Not to mention the mind-body connection and conditions like anxiety and depression impacting autonomic status.
As with any case, we must remember to treat the whole person and be sure we’re looking at all of the “symptom generators” of concussion and PCS.
Fancy Tools.
There are vagus nerve stimulators, cold plunge devices (e.g., parasympathetic diver’s reflex), etc. These must be recommended on a patient-by-patient basis based on clinician expertise and clinical indication. It’s not within the scope of this blog to provide an exhaustive list of potential autonomic rehabilitation tools and options.
Concluding Thoughts.
The “autonomic/physiologic” patient profile should look very familiar if you’ve been managing concussions for any period of time. The finding of exercise intolerance is so prevalent that Dr. John Leddy once said, “In 2020, you don’t need an MRI, fMRI, DTI, or a blood test to diagnose concussion. Put them on a treadmill or bike [to test exercise/autonomic tolerance]… Every 1bpm increase in heart rate threshold resulted in a 0.82 day shorter recovery.” (AAN 2020 Virtual Sports Concussion Conference).
That was four years ago, and the research has only reaffirmed this claim. Every patient who steps into your office deserves the due diligence of assessing their orthostatic and exercise tolerance. It’s the exact opposite of “rest until your symptoms go away” and will move the recovery needle further and faster than most other therapies in the concussion recovery toolbelt.
References
Fu, Q., & Levine, B. D. (2018). Exercise and non-pharmacological treatment of POTS. Autonomic neuroscience, 215, 20-27.
Leddy, J. J., Haider, M. N., Noble, J. M., Rieger, B., Flanagan, S., McPherson, J. I., … & Willer, B. (2021). Clinical assessment of concussion and persistent post-concussive symptoms for neurologists. Current neurology and neuroscience reports, 21, 1-14.
Leddy, J. J., Haider, M. N., Noble, J. M., Rieger, B., Flanagan, S., McPherson, J. I., … & Willer, B. (2021). Management of concussion and persistent post-concussive symptoms for neurologists. Current neurology and neuroscience reports, 21, 1-7.
Len, T. K., & Neary, J. P. (2011). Cerebrovascular pathophysiology following mild traumatic brain injury. Clinical physiology and functional imaging, 31(2), 85-93.
Pearson, R., Sheridan, C. A., Kang, K., Brown, A., Baham, M., Asarnow, R., … & Choe, M. C. (2022). Post-concussive orthostatic tachycardia is distinct from postural orthostatic tachycardia syndrome (POTS) in children and adolescents. Child Neurology Open, 9, 2329048X221082753.
Snowden, T., Morrison, J., Boerstra, M., Eyolfson, E., Acosta, C., Grafe, E., … & Christie, B. R. (2023). Brain changes: aerobic exercise for traumatic brain injury rehabilitation. Frontiers in Human Neuroscience, 17.