Not all whiplash injuries result in a concussion injury, but all concussion injuries will have a component of a whiplash injury. Your cervical spine, commonly known as your “neck,” is…
Concussions can happen to athletes of any age participating in all kinds of sports. From hard hits in hockey and football to accidents in gymnastics and soccer, concussions are an…
Greater Toronto Area’s Leading Multidisciplinary Clinics for Concussion Recovery
Concussions are a common form of traumatic brain injury, often caused by blows to the head. They can result in an array of physical, cognitive, and emotional symptoms that may…
Rethinking Concussion Recovery: The Case for Active Rehabilitation Concussions are more than just a bump on the head, or “getting your bell rung”; they are a type of mild traumatic…
Every patient with a concussion is a patient with a neck injury. Let me explain.
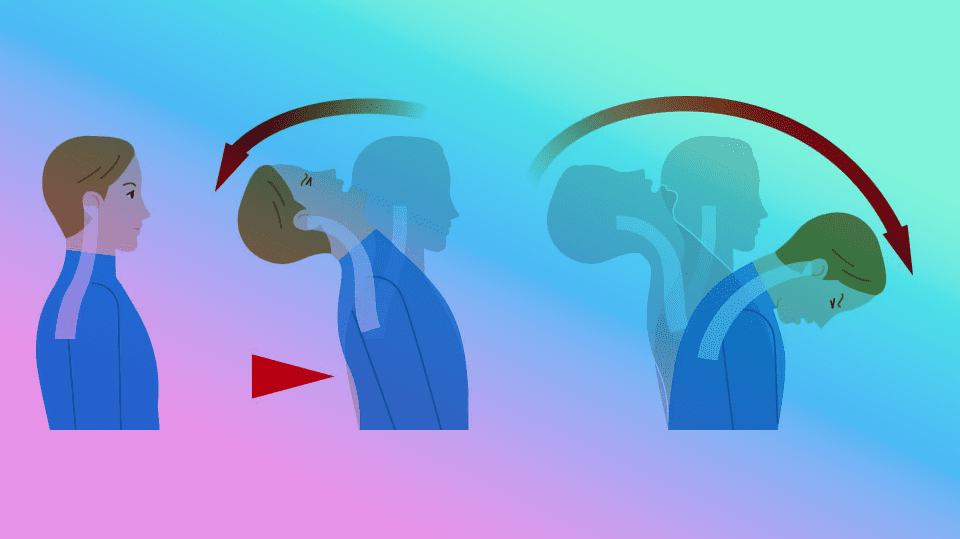
A concussion results when the brain undergoes such rapid acceleration-deceleration that shearing and stretching of neurons occur. But obviously, not every blow to the head or body, and not every instance of brain acceleration-deceleration (like, say, nodding “yes”) will result in concussion.
What is the force threshold for brain injury? How much force must be involved to cause a concussion? The answer is 60-160gs (measured in g-forces).
Now, that’s quite a lot of force (the g-forces withstood in flight by a fighter pilot reach about 9gs by comparison). However, a neck sprain/strain requires only 4.5gs of force to occur. The corollary is probably quite obvious.
When the head accelerates and then decelerates from a blow to the body or head, so does the neck. However, for the force of the acceleration-deceleration event to be sufficient for concussion, it must surpass the force threshold for a neck injury. While head and neck velocity after impact may differ, the difference will be relatively slight and insufficient to avoid deleterious effects on the cervical spine and its structures.
A Famous Case in Point.
Every patient who is assessed for concussion should also be assessed for — and ultimately treated for — neck pathology.
Here’s a famous case in point:
Midway through his 2010-2011 season, the Pittsburgh Penguins’ star player Sidney Crosby was diagnosed with a concussion. The ensuing months were disastrous. Plagued by persistent symptoms, Crosby was not able to return to play until the following season. Finally returning to play for the 2011-2012 season, he was placed back on the injured list when his symptoms returned after only eight games in.
It wasn’t until advanced imaging revealed signs of an upper cervical soft tissue injury that it became clear that, in fact, it likely was not a concussion that was prolonging his recovery. It was his neck.
A relatively short time after the new diagnosis and subsequent treatment, he returned to play the rest of the season.
Why did the Diagnosis get Missed?
What makes the neck diagnosis in a concussion patient so elusive is that the symptoms of concussion — headache, nausea, balance problems, dizziness, fatigue, blurred vision, brain fog — areidentical to that of whiplash. Clinicians need to recognize the significance of this symptom overlap and, moreover, that the mechanism of injury in concussion and in whiplash is essentially the same.
The cervical nerve roots, musculature in the cervical and thoracic spine regions, the trigemino-cervical nucleus, the intervertebral discs, and the zygapophyseal joints of the cervical and thoracic regions are potentially affected in a whiplash injury. As you can imagine, these structures together can cause a wide array of symptomatic expressions.
Assessing and Treating Post-Concussive Whiplash.
Ruling out red flags is always the most important part of any patient evaluation.
On the sideline,any neck pain or tenderness resulting from a concussive blow should be treated as a serious injury until proven otherwise.
Medical providers on the sideline should also consider any resultant weakness, tingling, burning, or numbness in 1) both arms and/or 2) one leg following a suspected concussion.
When red flags such as these are present on the playing field, the neck should be stabilized immediately, and the patient should be transported by ambulance until serious neck pathology is ruled out.
In the clinic, these symptoms should still be taken seriously, and the possibility of fracture should not be ruled out until an adequate history and physical examination have been conducted.
For a full list of concussion-related red flags, refer to theSCAT 6.
Ask About Neck-Specific Signs and Symptoms.
Is your patient experiencing neck pain or limitations in the cervical spine range of motion? Do they have occipital headaches or headaches that seem to originate in the neck?
Your patients may not have neck pain at the time of clinical presentation, but did they experience symptoms at the time of their injury?
It is also possible that patients will not be able to recall neck pain at any point since their concussion. However, this does not rule out a whiplash injury. Many times in my own practice, patients have denied any experience of neck pain, but physical exam almost always tells a different story. Personally, I cannot recall a time when simple palpation has not revealed suboccipital muscle tenderness, at the very least, in my concussed patients, particularly in acute cases.
If the patient is experiencing significant neck pain at the time of presentation, you would be wise to have them fill out an outcome measure such as theNeck Disability Index so that you may more objectively track their progress in the days, weeks, or months to come.
Check Range of Motion.
According to theCanadian C-Spine Rule, a limitation of active cervical spine rotation to less than 45 degrees may warrant further investigation with X-ray imaging. Combining what you learn from the range of motion testing with what your patient has told you about their current and past neck pain experience will help you make this determination.
Conduct a Thorough Physical Examination.
In all cases, orthopedic and neurological testing should be performed to evaluate for potential concomitant musculoskeletal or nerve pathology. This may include assessing for joint dysfunction, muscle tightness or weakness, and nerve root tension.
Generally, the three fundamental aspects of your neck physical exam (after neurological assessment) will be 1) assessment of cervical/thoracic spine range of motion, 2) palpation of muscular and bony structures, and 3) standard orthopedic procedures like the Spurling test (which evaluates for nerve root compression).
Consider also the “Big 3” tests recommended by neurologists when assessing for cervicogenic headache or dizziness.
These tests include:
The Cervical Flexion-Rotation Test assesses dysfunction at the C1-C2 motion segment which accounts for 50% of rotation in the cervical spine. This test helps to identify patients who suffer from cervicogenic headache.
The Smooth Pursuit Neck Torsion Test assesses for disturbances in eye movement and postural stability. Its purpose is to specifically identify those patients who suffer from cervicogenic dizziness versus other causes of dizziness like BPPV or Meniere’s disease.
The Cervical Joint Position Error Test assesses for proprioceptive abnormalities stemming from cervical spine dysfunction. When the neck is injured, interference of sensory information from the cervical spine to the head can occur, causing sensorimotor abnormalities and concurrent symptoms like headache and dizziness.
Consider Advanced Imaging.
If your clinical evaluation reveals significant red flags or an inability to rule out potential neck pathology, imaging options such as X-ray, MRI, or CT may be considered.
Determine the Diagnosis.
Once you have ruled out serious neck pathology and have completed your physical examination, you will need to refine your primary diagnosis.
A Whiplash-Associated Disorder (WAD) is categorized as follows:
WAD 0: no neck pain
WAD I: neck pain, stiffness, or tenderness only. No physical signs.
WAD II: neck complaints and musculoskeletal signs (e.g., muscle spasm, limited active range of motion).
WAD III: neurological signs (e.g., decreased deep tendon reflexes, weakness) in addition to neck complaints and musculoskeletal signs.
WAD IV: fracture or dislocation, in addition to any of the above presentations.
A diagnosis of WAD I is most common in concussion patients. However, it is possible to present with a more complex WAD, particularly if there has been a previous history of neck injury or underlying cervical spine pathology.
Treating the Cervical Spine.
According to the 2023Amsterdam consensus statement, cervicovestibular rehabilitation is indicated for athletes with neck pain, headaches, dizziness, and/or balance problems, especially if these symptoms have persisted for more than 10 days.
What Should be Included in a Treatment Plan for the Neck?
Obviously, this will depend on a practitioner’s scope of practice. Regardless, a multimodal approach will yield the best results.
As a foundation, consider implementing the following “3 S’s” of neck rehabilitation:
Spinal mobilization and/or manipulation
Mobilization refers to a low-velocity, low-amplitude therapeutic force applied to any joint or tissue of the body. Mobilizations are often (but not always) rhythmic in nature.
Manipulation refers to a high-velocity, low-amplitude therapeutic force applied to any joint or tissue of the body.
Early mobilization of the cervical facet joints can be a safe and effective way to improve neck mobility and decrease pain. Later on, spinal manipulation may also be of significant benefit. However, there is a caveat.
Because concussion often results in abnormal blood flow to the brain as the result of dysregulation of the autonomic nervous system, it is best practice to wait at least one week before performing spinal manipulation on patients with concussion.
Spinal manipulation has been shown to increase blood flow to the brain. This is generally a good thing! But in the case of a concussed individual in whom cerebral blood flow may be off-kilter, the stimulus and subsequent autonomic effect of manipulation may further exacerbate symptoms.
Though spinal manipulation (especially of the neck) sometimes gets a bad rap due to worries about its safety, there is no proven indication in the scientific literature that it is a higher risk treatment for a majority of the patient population than, say, NSAIDs. As one group of researchers observe, “Though millions of [cervical spine manipulations] are performed without [adverse events], the results suggest that there is a very small but inherent risk associated with [cervical spine manipulation] even after a thorough examination for contraindications and proper clinical reasoning.”
Every therapeutic intervention comes with some degree of risk. But we should never downplay the risks of any treatment; nor should we exaggerate them. When it comes to spinal mobilization and manipulation, the bottom line is that the trained clinician who delivers mobilization or manipulation must always screen for contraindications, be cognizant and respectful of patient preferences, and assess carefully on a patient-by-patient basis to determine who is best suited for either therapy.
(For those interested in reading more about the safety and efficacy of neck manipulation, read thiscomprehensive ten-year study published in the estimable Spine journal.)
Strengthening exercises
Along with the mechanical damage of soft tissues incurred by a forceful injury to the neck, there may also be resultant neuromuscular dysfunction. Joint dysfunction may also emerge as a secondary effect from such soft tissue injuries. As one group of researchersput it:
“Abnormal signals from mechanoreceptors of injured capsules, ligaments, or anular [sic] fibers may cause corrupted neck muscle response patterns and hinder proper neck proprioception of whiplash patients. The neuromuscular control system may stiffen the injured neck to prevent further injuries, thus reducing active neck motion and causing painful muscle spasm.”
As such, strengthening and proprioceptive exercises will often play a major role in post-concussion rehabilitation.
Some of the muscles most commonly affected by whiplash include the suboccipital muscles, sternocleidomastoids, semispinalis capiti, and the deep neck flexors. Given the post-traumatic muscle spasm that may develop and the postural alterations that may correlatively ensue, stretching and strengthening exercises for the anterior and posterior thoracic region should also be considered.
Soft tissue therapy and/or stretching
Some of the muscles most likely to be affected by a whiplash injury include the suboccipital muscles, sternocleidomastoids, levator scapulae, trapezius, and the deep flexors of the neck.
Important postural muscles like the pecs, rhomboids, and subscapularis should not be overlooked.
A positive correlation has been seen in whiplash patients who undergo myofascial treatments as part of a multimodal rehab plan. For example, Dehner et al. found soft tissue and trigger point treatments to be associated with lower median periods of disability. In terms of reducing pain, the same study found these kinds of soft tissue therapy to be significantly more effective than passive therapy (e.g., heat, massage, electrotherapy) two months post-injury.
Preventing Neck Injuries.
Several studies have investigated the importance of neck muscle strength, stiffness, and endurance in mitigating neck injury risk associated with concussion. Neck stiffness appears to be the most important factor here. However, it must still be emphasized that concussions often occur when there is not enough reaction time to stiffen the neck voluntarily before the concussive blow to the head, neck, or body.
What does this mean? Given the nature of sport and the context within which concussions often occur in sport, the best way to mitigate concussion risk in real life is greater game awareness.
In Conclusion
As was stated at the onset, every patient with a concussion is a patient with a neck injury. The field of contemporary concussion management is rapidly shifting away from a myopic focus on the head to include an understanding of the importance of diagnosing and treating neck injuries that often occur concomitantly with concussion (not to mention other systems of the body).
This emphasizes the core underlying principle of concussion management, namely, that the best approach must be multimodal in nature. No single intervention is likely to be a panacea. Instead, the best results are obtained when concussion treatment protocols address not strictly the brain or body but the whole person in all his or her systems: from the neurological to the psychological and everything in between.
Sources:
Curatolo M, Bogduk N, Ivancic PC, McLean SA, Siegmund GP, Winkelstein BA. The role of tissue damage in whiplash-associated disorders: discussion paper 1. Spine (Phila Pa 1976). 2011 Dec 1;36(25 Suppl):S309-15.
Dabbs, V, and W J Lauretti. “A risk assessment of cervical manipulation vs. NSAIDs for the treatment of neck pain.” Journal of manipulative and physiological therapeutics vol. 18,8 (1995): 530-6.
Dehner C, Elbel M, Strobel P, et al. Grade II whiplash injuries to the neck: What is the benefit for patients treated by different physical therapy modalities? Patient Saf Surg. 2009;3:2.
Haldeman S et al, Clinical Practice Implications of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders: From Concepts and Findings to Recommendations. Spine 33(4S):p S199-S213, February 15, 2008.
Leddy, John J et al. “Clinical Assessment of Concussion and Persistent Post-Concussive Symptoms for Neurologists.” Current neurology and neuroscience reports vol. 21,12 70. 24 Nov. 2021.
Leslie O., Craton N. Concussion: Purely a brain injury? Clin. J. Sport Med. 2013;23:331–332.
Marshall, Cameron M et al. “The role of the cervical spine in post-concussion syndrome.” The Physician and sportsmedicine vol. 43,3 (2015): 274-84.
Meaney DF, Smith DH. Biomechanics of concussion. Clin Sports Med. 2011 Jan;30(1):19-31, vii.
Puentedura EJ, March J, Anders J, Perez A, Landers MR, Wallmann HW, Cleland JA. Safety of cervical spine manipulation: are adverse events preventable and are manipulations being performed appropriately? A review of 134 case reports. J Man Manip Ther. 2012 May;20(2):66-74.
Teasell RW, McClure JA, Walton D, Pretty J, Salter K, Meyer M, Sequeira K, Death B. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 2 – interventions for acute WAD. Pain Res Manag. 2010 Sep-Oct;15(5):295-304.
Vendrig, Alexander A. PhD; van Akkerveeken, Pieter F. MD, PhD; McWhorter, Kevin R. PT. Results of a Multimodal Treatment Program for Patients With Chronic Symptoms After a Whiplash Injury of the Neck. Spine 25(2):p 238, January 15, 2000.
Dr. Matthew Nelson is a graduate of the University of Regina (Physical Education, 2007) and the Canadian Memorial Chiropractic College (2014) where he graduated with Clinic Honours and was the recipient of the Istrati Family Memorial Award. He is currently pursuing an MA in Philosophy at Holy Apostles College and Seminary.
Matt played football for the University of Regina Rams for four seasons. Following his time with the Rams, he trained for one year in Bobsleigh Canada Skeleton’s development program. He is owner and clinician at Core Health + Performance in Shaunavon, Saskatchewan. He is married and the father of four children.