Concussions can happen to athletes of any age participating in all kinds of sports. From hard hits in hockey and football to accidents in gymnastics and soccer, concussions are an…
Greater Toronto Area’s Leading Multidisciplinary Clinics for Concussion Recovery
Concussions are a common form of traumatic brain injury, often caused by blows to the head. They can result in an array of physical, cognitive, and emotional symptoms that may…
Why You Should Never Skip the Neck in Concussion Evaluation & Rehab.
Every patient with a concussion is a patient with a neck injury. Let me explain. A concussion results when the brain undergoes such rapid acceleration-deceleration that shearing and stretching of…
Rethinking Concussion Recovery: The Case for Active Rehabilitation Concussions are more than just a bump on the head, or “getting your bell rung”; they are a type of mild traumatic…
Every suspected traumatic brain injury warrants a thorough neurological examination. As you conduct your exam, it is important to remember that a brain injury may include structural or functional compromise of the nerves exiting the brain (or their nuclei within the brain). Thus, the cranial nerve exam will be an essential element of your neurological assessment.
Practitioners sometimes find the cranial nerve (CN) exam intimidating due to the complexity of the anatomy involved and the clinical sophistication that the exam demands from the clinician carrying it out. However, with a systematic approach to the exam — and a little bit of practice — it is possible to accurately and efficiently assess the function of each cranial nerve without difficulty.
Before we explain how to do that, let’s review some relevant anatomy.
Anatomy Review.
The cranial nerves are bundles of sensory and/or motor fibres that 1) innervate muscles, 2) innervate glands, or 3) carry afferent nerve signals to the central nervous system from sensory receptors.
Of these nerves, there are twelve pairs. They are called “cranial” nerves because they emerge from the cerebrum, cerebellum, or brainstem and pass distally through openings in the cranium. Passing through the cranium, they are covered by sheaths derived from the cranial meninges.
Unlike spinal nerves, whose roots are neural fibers from the spinal grey matter,cranial nerves are composed of the neural processes associated with distinct brainstem nuclei and cortical structures.
As a general rule, the more posterior and lateral nuclei tend to be sensory, and the more anterior tend to be motor.
Cranial nerves I, II, and VIII are considered purely afferent (i.e., sensory).
Cranial nerves III, IV, VI, XI, and XII are purely efferent (i.e., motor).
The remaining cranial nerves, V, VII, IX, and X, are functionally mixed (i.e., sensory and motor).
It is essential that clinicians have a good understanding of the anatomical structures they are testing during clinical procedures like the CN exam. This ensures more precise assessments and more reliable results so that abnormalities causing neurological symptoms will be identified and promptly acted upon.
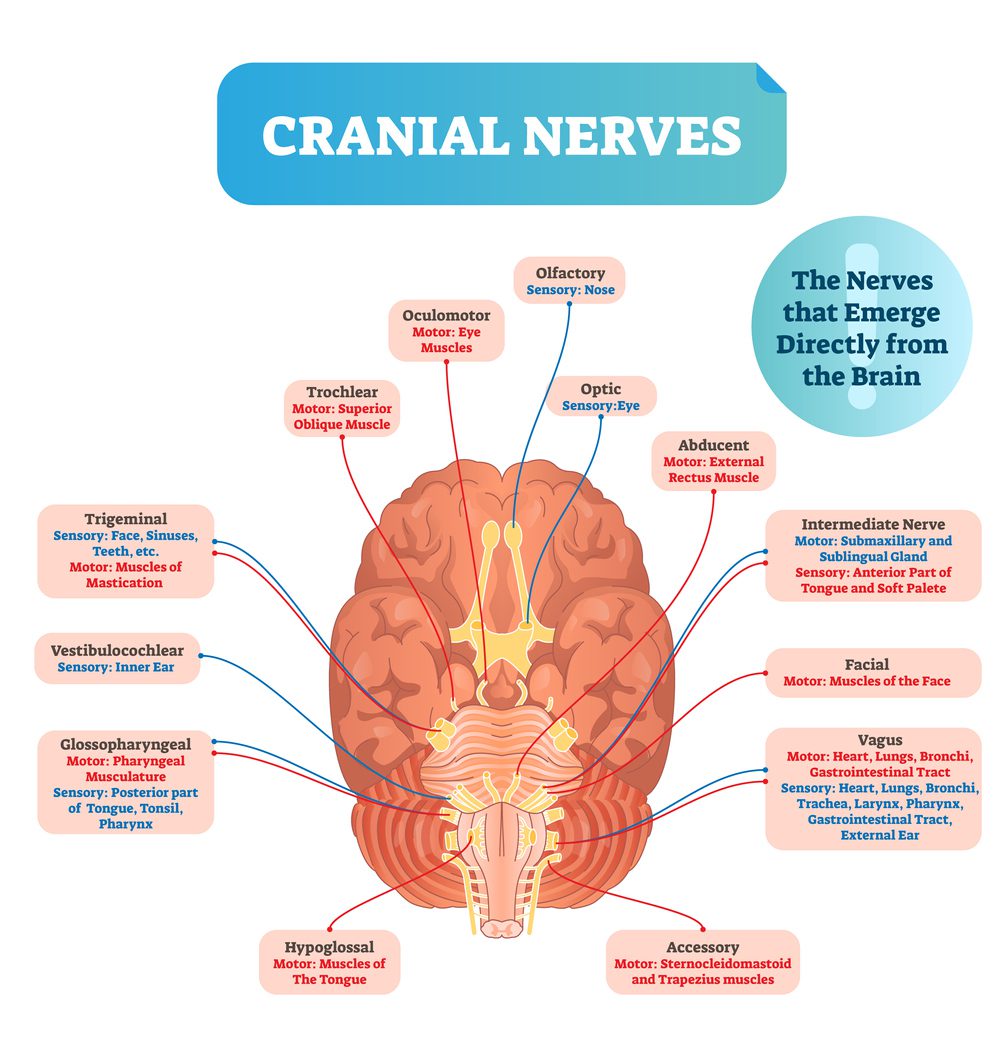
Before reading ahead, take a few minutes to review the following diagram:
Cranial nerves vector illustration.
The Twelve Cranial Nerves.
Understanding how to test a particular nerve requires understanding what that particular nerve does. One must understand proper function to detect dysfunction in a physiological structure or system.
What specifically is the proper function of each cranial nerve? After reading through this list, run through it again and test yourself on each nerve’s number, name, and function(s):
CN I
The Olfactory Nerve
Responsible for the sense of smell (olfaction)
CN II
The Optic Nerve
This is the “seeing” nerve as it carries visual signals from the retinae to the brain
CN III
The Oculomotor Nerve
Controls eye movements and pupil size
CN IV
The Trochlear Nerve
Controls eye movement and pupil size
CN V
The Trigeminal Nerve
Carries sensory information from the face and the mouth and innervates “chewing” muscles
CN VI
The Abducens Nerve
Carries motor signals responsible for lateral eye movement (eye abduction)
CN VII
The Facial Nerve
Carries signals that control facial muscles and the lacrimal gland, which produces tears
CN VIII
The Vestibulocochlear Nerve
Responsible for auditory and equilibrium sensations, or put more simply, hearing and balance
CN IX
The Glossopharyngeal Nerve
Carries signals from the throat and tongue and is responsible for things like taste at the back of the tongue and the gag reflex
CN X
The Vagus Nerve
Responsible for controlling the muscles of the pharynx, larynx, and diaphragm. It also carries afferent signals to the brain from many organs, including the heart and lungs
CN XI
The Spinal Accessory Nerve
Carries signals to the neck and shoulder muscles
CN XII
The Hypoglossal Nerve
Controls tongue movements
The Cranial Nerve Exam: A Walk-Through
Now, let’s look at how to test each nerve listed above. The following test descriptions are laid out according to the anatomical order of the cranial nerves, from CN I to XII.
NOTE: You do not necessarily need to follow this order when conducting your tests. Be creative! Think about how you can order your tests to 1) improve flow, 2) make the tests easier to remember, and 3) make your exam more efficient. (Here isone example of how you might administer the tests.)
The cranial nerve exam process includes the following:
Observation:
Start by observing the face, neck, and torso for bruising, swelling, spasms, asymmetry, and/or other involuntary movements.
Olfactory Nerve (I):
Test both nostrils independently.
Ask the patient if he has noticed any changes to his smell.
Assess the patient’s sense of smell by asking him to identify common smells (e.g., coffee, soap, cloves, mint) with his eyes closed. Have the patient cover each nostril and test each side independently for asymmetry.
Optic Nerve (II):
A. Examine the patient’s visual acuity with a Snellen chart. The chart may be on a screen (via an eye exam app) or on paper. Keep the chart 30–40 cm from the patient and assess each eye’s acuity individually (as the patient covers each eye).
Eye test chart.
B. Test the visual field in all four quadrants. Cover the same eye as your patient. Tell your patient to stare at your nose during the visual field test. Wiggle your finger as you move it from the periphery toward the midline in all quadrants, and have your patient say “yes” whenever he sees your wiggling finger. Look for any glaring deficits or asymmetries in peripheral vision.
C.(Optional) If you have one on hand, You can inspect the optic disc with an ophthalmoscope.
Oculomotor, Trochlear, and Abducens Nerves (III, IV, VI):
A. Observe the patient’s pupils for size, shape, and symmetry. Note any irregularities.
B. Tests the pupils’ direct and indirect reactions to light. Shine a penlight into one eye and note the dilation—the “direct response.” At the same time, note whether the other eye also dilates—the “indirect response.” Test both eyes.
C. Conduct an H-pattern test for eye movement:
Have the patient follow finger movements with eyes only while keeping their head still.
Move your finger in an “H” pattern (up and down, left and right) in front of the patient.
Look for eye deviation, abnormal head posture, nystagmus, or jerky movements as you move your fingers.
D. Test convergence by moving a penlight toward the bridge of the patient’s nose at the end of the H-pattern test, noting any asymmetries or aberrations as eyes move medially.
E. (Optional) You may decide to test saccades. Do this by facing your patient, standing no more than 1 meter away. Place your fingers 1.5 feet from the midline (3 feet apart). Ask the patient to keep their head still while looking back and forth from one finger to another as quickly as possible, ten times in a row. The head should remain still. Note any involuntary head movements, any over or undershooting of the target finger, or any latency.
Trigeminal Nerve (V):
Recall that the trigeminal nerve has motor and sensory functions.
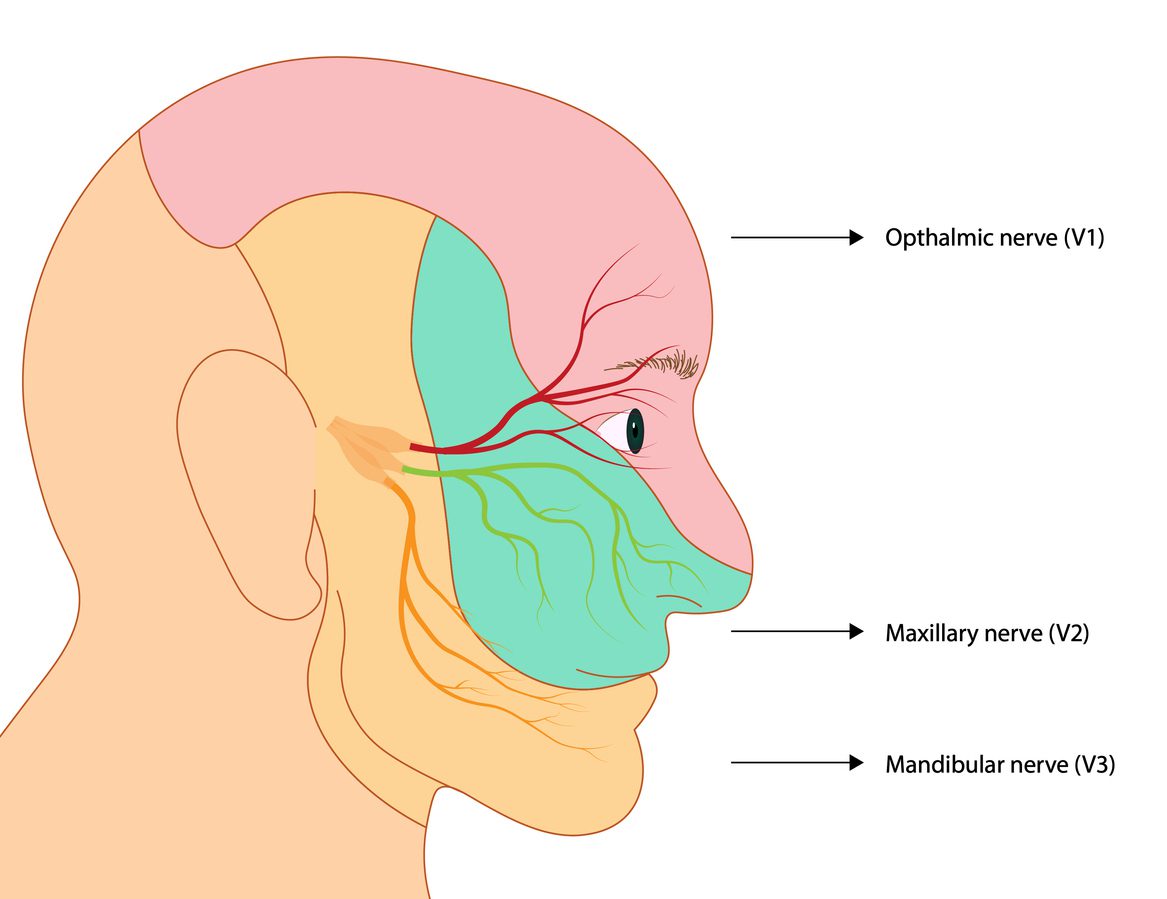
A. Test facial sensations using two simple tools: a dull object (e.g., eraser tip or ball) and a sharp object (e.g., paper clip or tweezers). Be sure to test all three divisions of the trigeminal nerve — ophthalmic, maxillary, and mandibular — with both objects.
Ask the patient to close their eyes. As you apply the objects to all three regions of the face, have the patient indicate whether the object is “sharp” or “soft.”
Trigemial nerve illustration. Ophtalmic, Maxillary and mandibular nerve
A. Test corneal reflex by having the patient hold their eyes open while you gently touch each eye with a cotton swab; note if the patient blinks.
B. Test motor function of the trigeminal nerve by having the patient open mouth against resistance and assess for weakness. Also, look for jaw deviation on opening. Finally, palpate for masseter asymmetry.
Facial Nerve (VII):
A. Observe the symmetry of the face at rest and during movement.
B. Test facial muscles by asking the patient to perform various facial expressions, such as smiling, frowning, raising eyebrows, puffing out cheeks, showing teeth, and closing eyes tightly.
C. (Optional) Test taste on the anterior 2/3 of the tongue with sweet, sour, or salty solutions.
Vestibulocochlear Nerve (VIII):
A. Screen for hearing loss by standing behind the patient and rubbing fingers together lightly on the right or left side of the patient’s head while asking the patient to locate which side they hear the rubbing. Do this enough times to determine whether one side or the other is inhibited (rule out the possibility of lucky guesses!). A slight variation is to whisper something on each side and have the patient repeat it back to you.
B. To further test hearing, perform the Weber and Rinne tests using a 512 Hz tuning fork:
For the Weber test, place the base of the tuning fork on the patient’s forehead or midline vertex while asking if the sound is heard equally in both ears.
For the Rinne test, place the base of the tuning fork on the mastoid process (testing bone conduction) and then near the auditory meatus (testing air conduction). Air conduction should be twice as long as bone conduction. Again, ask if the sound is heard equally in both ears.
If bone conduction is heard longer than air conduction, this indicates that the patient has conductive hearing loss.
If air conduction is heard longer than bone conduction – but not twice as long – then it may indicate sensorineural hearing loss.
B. (Optional) You may also check for nystagmus. If you suspect vestibular pathology, consider performing the head thrust and/ or the Dix-Hallpike maneuvers. Keep in mind: symptoms like nystagmus and nausea may also be indicative of stroke. If you are concerned about the possibility of a stroke, you may do a Head Impulse-Nystagmus-Test of Skew (or HINTS) exam.
Note: you should never have to perform a HINTS and a Dix-Hallpike on the same visit.
Glossopharyngeal Nerve (IX):
Observe for any asymmetry or weakness in swallowing (assess current diet, difficulty managing secretions). Keep in mind that CN XII (Vagus Nerve) also innervates structures involved in swallowing.
Assess the patient’s gag reflex with a tongue depressor.
Optional: test taste on the posterior 1/3 of the tongue by asking the patient to identify bitter flavors.
Vagus Nerve (X):
Assess the patient’s voice for hoarseness, weakness, or nasal quality.
Ask about any difficulty with speaking, swallowing, or breathing.
Spinal Accessory Nerve (XI):
Injury to the spinal accessory nerve can lead to dysfunction of the trapezius and sternocleidomastoid. As a major scapular stabilizer, dysfunction of the trapezius can lead to pain and disability.
Look for a drooping shoulder, winging of the scapula, and other shoulder asymmetry.
Test for weakness in shrugging shoulders (trapezius) and turning the neck (SCM).
Ask about any difficulty with movement or strength in neck muscles and check neck rotation against resistance (assessing the SCM).
Hypoglossal Nerve (XII):
Have the patient stick out their tongue and observe for any asymmetry, atrophy, or fasciculations.
Ask the patient to push the tongue against the inside of the cheeks and check against resistance for strength.
Closing Considerations.
Conducting a thorough and systematic cranial nerve assessment is essential in evaluating the health of an individual’s central nervous system. It can provide valuable information about potential underlying conditions and help identify specific areas for further evaluation and treatment. In the case of concussion, any cranial nerve irregularities discovered in the post-injury exam should be thoroughly evaluated, and when necessary, prompt referral should be arranged.
Remember that many pathologies may explain cranial neuropathies. Aside from traumatic head injury, other possible causes are diabetes, high blood pressure, infection, and tumors. They can also be idiopathic. Always consider these when formulating your differential diagnoses.
Moreover, it is crucial to consider the patient’s history, medications, and overall health when assessing cranial nerve function. Certain conditions and medications can affect the functioning of the nerves, so it is important to have a comprehensive understanding of the patient’s medical background.
Furthermore, it is important to remember that while the tests described above can help with initial screening, they should not be used as the sole basis for diagnosis. Not every positive test means underlying clinically significant pathology. A thorough history, careful physical examination, and appropriate medical imaging are all crucial in making an accurate diagnosis and determining the appropriate treatment plan. Consultation with a neurologist may be necessary for more complex cases.
Though perhaps daunting in scope and complexity, you will inevitably master the cranial nerve examination with careful and consistent practice. Few aspects of the physical examinations provide so much information to the clinician so quickly, and you will find this exam incredibly useful in your everyday practice and not merely with your concussion patients. After all is said and done, acquiring the art of the cranial nerve exam is undoubtedly worth your time, effort, and the inevitable pains that come with learning hard things.
REFERENCES:
Coello AF, Canals AG, Gonzalez JM, Martin JJ. Cranial nerve injury after minor head trauma. J Neurosurg. 2010;113:547-555.
Moore, K. L., Dalley, A. F., & Agur, A. (2006). Clinically oriented anatomy (5th ed.). Lippincott Williams and Wilkins.
Newman, George. How to do the Cranial Nerve Examination. Sridhara S. Yaddanapudi, MD. Department of Neurology, Einstein Medical Center, Philadelphia, PA
Reese V, M Das J, Al Khalili Y. Cranial Nerve Testing. [Updated 2023 May 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK585066/
Taylor A, Mourad F, Kerry R, Hutting N. A guide to cranial nerve testing for musculoskeletal clinicians. J Man Manip Ther. 2021 Dec;29(6):376-389.
Walker NR, Mistry RK, Mazzoni T. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jul 4, 2023. Facial Nerve Palsy.
Sonne J, Lopez-Ojeda W. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Dec 9, 2022. Neuroanatomy, Cranial Nerve.
Dr. Matthew Nelson is a graduate of the University of Regina (Physical Education, 2007) and the Canadian Memorial Chiropractic College (2014) where he graduated with Clinic Honours and was the recipient of the Istrati Family Memorial Award. He is currently pursuing an MA in Philosophy at Holy Apostles College and Seminary.
Matt played football for the University of Regina Rams for four seasons. Following his time with the Rams, he trained for one year in Bobsleigh Canada Skeleton’s development program. He is owner and clinician at Core Health + Performance in Shaunavon, Saskatchewan. He is married and the father of four children.