Three Tools That Clinicians Can Use to Optimize Their Concussion Treatment Plan As a healthcare provider, treating concussions can be challenging. There are a lot of different interacting systems that…
How to Strengthen Cervical Muscles After a Concussion or Whiplash
Not all whiplash injuries result in a concussion injury, but all concussion injuries will have a component of a whiplash injury. Your cervical spine, commonly known as your “neck,” is…
Concussions can happen to athletes of any age participating in all kinds of sports. From hard hits in hockey and football to accidents in gymnastics and soccer, concussions are an…
Greater Toronto Area’s Leading Multidisciplinary Clinics for Concussion Recovery
Concussions are a common form of traumatic brain injury, often caused by blows to the head. They can result in an array of physical, cognitive, and emotional symptoms that may…
Concussions are a subset of mild traumatic brain injuries (mTBIs), and are characterized by temporary disruptions in brain function, resulting from external kinetic forces applied to the head or body. This intricate pathophysiological process commences as the sudden acceleration or deceleration of the brain within the cranial vault triggers a cascade of ionic, metabolic, and physiologic disturbances. Following a concussive event, the brain experiences a disruption in normal cellular processes, including alterations in neurotransmitter release, impaired cerebral blood flow, and energy imbalances. These changes can precipitate a wide range of clinical symptoms, warranting a nuanced understanding among healthcare providers for accurate diagnosis, management, and guidance on the prognosis of those affected by this type of brain injury.
During these high-energy events, the brain experiences inertial forces, causing it to move back and forth or twist within the cranial vault. This rapid motion can lead to a complex series of physical and biochemical changes within the brain. The acceleration/deceleration movement is particularly associated with rotational forces that contribute to the severity of the concussion.
Common Symptoms.
Concussions can lead to both physical and cognitive impairment, and symptoms can include but are not limited to, headache, confusion, dizziness, visual disturbances, memory impairment, other cognitive deficits, and emotional instability. Clinicians should be vigilant in identifying a spectrum of cognitive, physical, emotional, and sleep-related symptoms that are suggestive of a concussion.
What Happens to the Brain?
The immediate aftermath of such a kinetic impact is the stretching or shearing of neurons and other neural structures. This mechanical disruption can produce a variety of neuropathological events. The axonal damage, referred to as diffuse axonal injury (DAI), can lead to disorganized ion flow and altered metabolic processes in neurons [1].
Neurometabolic Changes.
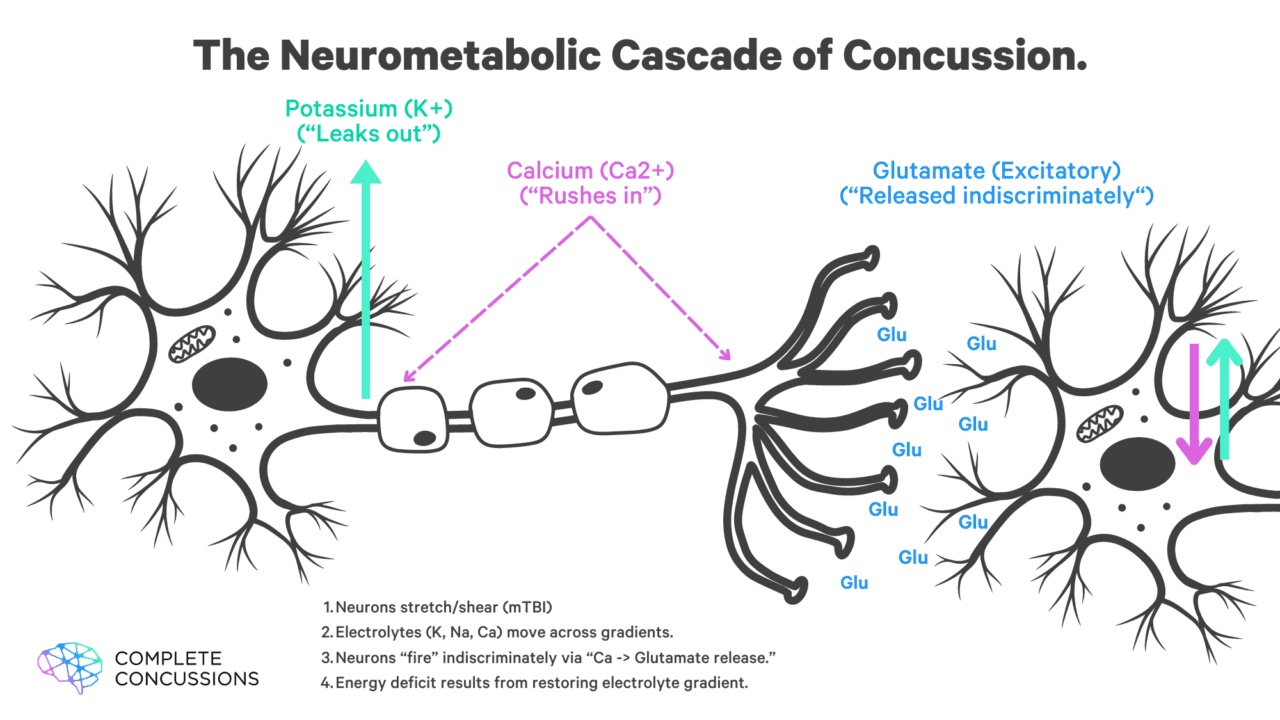
Following the mechanical insult, there is a period of altered neurometabolic activity, which may last from minutes to days. One hallmark of concussion is ionic flux. This occurs when axons in the brain are stretched, opening up pores in the membrane of these cells, resulting in the efflux of potassium and influx of calcium and sodium. This rapid exchange of ions results in depolarization (“activation”) of the neuron and subsequent action potentials, which then results in the release of excitatory neurotransmitters like glutamate, leading to further depolarization of additional neurons and more action potentials. This widespread, haphazard firing of neurons results in the “excitatory” phase of concussion. This disruption in the normal balance of ions inside and outside of the cell contributes to a state of metabolic crisis. At the same time, the brain works to restore the ionic balance and neuronal membrane integrity [1].
Active Transport and the Demand for ATP.
Once the normal concentration of ions required to maintain resting membrane potential has been altered, the brain must work to restore it actively. It uses active (ATP-dependent) transport to pump sodium and calcium out of the cell and potassium into the cell [2]. This process requires considerable amounts of ATP, the body’s energy molecule. In a normal, healthy brain, about two-thirds of all ATP is used to maintain the normal concentration gradient of ions on either side of the cell membrane. In an injured brain, this is, of course, increased.
(Image adapted from Giza and Hovda 2014)
The Consequences of Calcium.
After the initial traumatic axonal injury occurs, resulting in an influx of calcium into the neuron, there is a second mechanism by which a further influx of calcium occurs. Once the axon has been depolarized, it releases the excitatory neurotransmitter glutamate, which then binds to N-methyl-d-aspartate (NMDA) receptors on the cell membrane, resulting in the opening of voltage-gated calcium channels and large amounts of calcium flooding into the cell [1]. This massive influx of calcium into the cell is accommodated by sequestering it in the cell’s mitochondria, which calcium has a high affinity for [1]. However, this can result in mitochondrial dysfunction, impairing their ability to create ATP via oxidative metabolism (normally, mitochondria can convert one glucose molecule into 34-38 ATP) [1]. Consequently, the brain must switch to anaerobic metabolism to create ATP. This process is nine times less efficient and also results in the generation and buildup of reactive oxygen species, which can lead to cellular damage [2]. Thankfully, in the context of mild traumatic brain injury, the body’s antioxidant systems can suppress this buildup and avoid any permanent cellular damage. However, this is not typically the case in moderate or severe TBI. In addition to disrupting mitochondrial function, calcium may also cause damage to axonal microcellular structures such as microtubules and neurofilament side arms, leading to impaired function [1].
Research has demonstrated that the increased intracellular calcium concentration tends to last longer than the increased intracellular and extracellular concentrations of sodium and potassium, respectively [1].
Supply, Demand and the Energy Crisis.
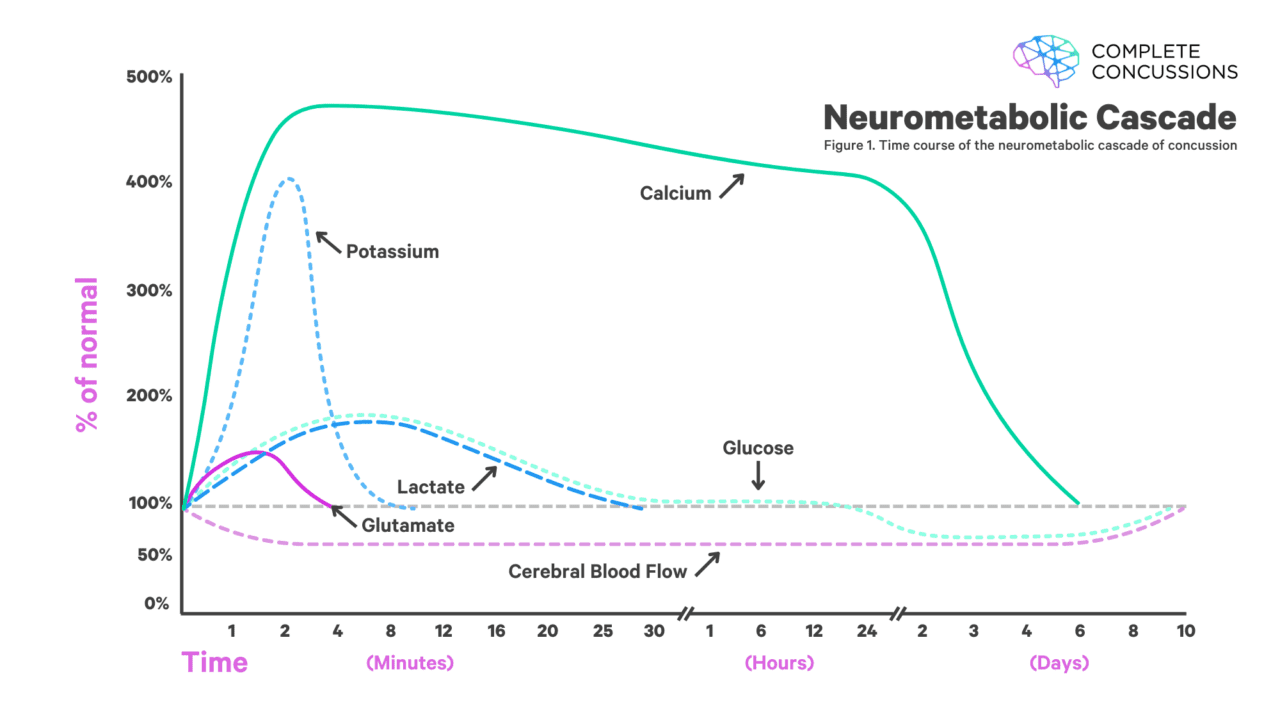
The increased demand for ATP to help restore resting membrane potential, coupled with the impaired ability of the brain to produce it, results in a metabolic energy crisis that can last up to 30 days in humans. Further contributing to this energy crisis is a reduction in blood flow to the brain, which provides the glucose that is then converted into ATP to use for cellular processes [1][2].
Magnesium As a Preventative Tool?
In addition to the previous neurometabolic changes, studies have shown a reduction in intracellular magnesium in the first four days following concussion. This reduction in magnesium levels is correlated with post-injury neurological deficits due to various mechanisms (i.e., Mg is involved in the normal function of over 300 enzymes). Specific to traumatic brain injury, in animal experiments, treatment with magnesium has resulted in improved motor performance [3]. Magnesium also competes with calcium at the NMDA receptor. If magnesium can bind to NMDA receptors, it acts as a “plug” to block calcium. Thus, as mentioned earlier, it can reduce the influx of calcium into the cell, which would occur via the opening of the voltage-gated calcium channels. Many people worldwide are deficient in magnesium, particularly athletes who lose larger amounts of magnesium in their sweat [10]. Therefore, supplementing with magnesium may hasten recovery time from concussion and reduce injury severity by limiting the extent of calcium influx and aiding the mitochondria in producing more ATP to restore normal ionic balance in the brain.
(Image adapted from Giza and Hovda 2014)
Blood Flow.
In recent years, extensive research has examined changes in cerebral blood flow following traumatic brain injury. These alterations are critical to understanding the consequences of concussions and the challenges they pose to recovery.
Immediate Changes in Cerebral Blood Flow.
Immediately after a concussion, there is a decrease in blood flow to the brain [4]. This disruption, along with potential changes in the regulation of cerebral blood flow, can contribute to the symptoms experienced immediately after head trauma. Animal studies have shown a reduction in cerebral blood flow of 50% within 1 hour following a concussion injury, and a 2018 study of concussed collegiate athletes found significantly lower blood flow 24-48 hours post-injury in multiple regions of the brain [5]. Several other human studies have shown that blood flow impairments can last up to 30 days, even in individuals who are no longer exhibiting symptoms [6] [7].
Persistent Impairment in Cerebral Blood Flow.
In some patients, impaired cerebral blood flow can persist long after the initial injury. This ongoing irregularity in blood flow is often associated with dysfunction of the autonomic nervous system, which regulates various unconscious functions, including heart rate and blood pressure. These dysfunctions can affect blood vessel dilation and constriction, leading to sustained abnormal blood flow patterns [4].
Symptoms stemming from this impaired blood flow can manifest as headaches, dizziness, and other post-concussive symptoms that interfere with daily activities and quality of life. Such symptoms indicate that the brain is still vulnerable and requires more time to fully recover.
Mechanisms of Blood Flow Regulation.
There are four primary mechanisms by which blood flow within the brain is regulated.
Cerebral Autoregulation
This describes the ability of the autonomic nervous system to react to changes in systemic blood pressure. The vasculature within the brain is very sensitive to changes in blood pressure. It will normally relax in response to low blood pressure and constrict in response to higher blood pressure to maintain stable blood flow, though the exact mechanism by which this occurs is still unknown. Research has demonstrated that this autoregulation is very sensitive to trauma or damage and is impaired in the context of concussive brain injury.
Cerebrovascular Reactivity
This describes the changes in cerebral blood flow in response to changes in partial pressures of CO2. If the concentration of blood carbon dioxide increases, cerebral vasculature will dilate to increase blood flow in an attempt to increase oxygen levels in the brain [6]. This is most heavily impacted by our breathing rate, with hyperventilation resulting in increased blood oxygen concentration and hypoventilation resulting in increased CO2 concentration. This has important implications in the context of concussion, as breathing rate has been shown to be impacted following concussion, with hyperventilation often being present, leading to increased CO2 concentration. A 2021 study concluded that symptom exacerbation during exercise in concussed patients may be mediated by increased sensitivity to cerebral vasculature to exercise-related increases in CO2 [14].
Neurovascular Coupling
This is the phenomenon by which blood is shunted to different areas of the brain based on increased activity in those regions. While research on this phenomenon in the context of concussion is somewhat limited, a 2016 study demonstrated that the failure to match cerebral blood flow with the metabolic demands of a region of the brain can lead to temporary or permanent alterations in neurological functioning [6]. This is often visualized using functional MRI (fMRI) but is almost exclusively done in the context of research rather than clinical assessment and care.
Neuroautonomic Cardiovascular Regulation
This refers to the coupling of the autonomic nervous system and the cardiovascular system and is typically reflected in our heart rate variability (HRV). High HRV is a marker of better health and indicates an improved ability of the body to adapt to many different changes. Increased sympathetic nervous system (our fight or flight mode) activity results in less heart rate variability, and this has important implications in the context of concussion, as it is well established that sympathetic nervous activity is increased following brain injury and parasympathetic nervous system (rest and digest mode) activity is suppressed. This can pose clinical challenges as patients may be symptom-free at rest or even with lighter exertion despite having these functional deficits in blood flow regulation. This highlights the importance of exertional testing, like the Buffalo Concussion Treadmill Test and Chicago Blackhawks Test, when looking to clear patients for return to situations with a high risk of head injury, such as contact sports.
Consequences of Repeated Concussions.
Additional risks arise when an individual sustains a second concussion before fully recovering from the first one. This situation can lead to second impact syndrome, a rare but potentially fatal condition characterized by rapid and severe brain swelling [11]. One of the hypothesized mechanisms behind second impact syndrome is that when the brain has not yet healed from an initial concussion, a second injury— even one that might otherwise be considered mild — can result in further impairment or loss of cerebral autoregulation. This may result in a disproportionate response in blood flow, leading to increased pressure and swelling which further damages already sensitive brain tissues. This highlights the serious risk of sustaining multiple concussions before the brain has fully physiologically recovered.
Recognizing and Addressing Blood Flow Changes.
The research findings on blood flow underscore the importance of timely and accurate assessment following a concussion. Monitoring and managing cerebral blood flow can be crucial in guiding treatment and determining the appropriate duration for recovery before resuming activities that carry a risk of head injury.
Advancements in imaging technology, such as functional MRI and CT perfusion, provide deeper insights into blood flow patterns in the brain post-concussion. These tools can help medical professionals evaluate the extent of a concussion and create more effective, individualized treatment plans that account for blood flow abnormalities.
Continued research into cerebral blood flow post-concussion not only helps in the management of acute symptoms but also has implications for preventing long-term damage associated with traumatic brain injuries. It is essential for individuals who have sustained a concussion to follow medical advice on relative rest, activity modification, and gradual return to activities to avoid complications related to altered blood flow and ensure a safe recovery.
The Blood-Brain Barrier and Concussion.
The blood-brain barrier acts as a selective filter protecting the brain from potentially harmful substances in the bloodstream while still allowing essential nutrients to pass through. After a concussion, this barrier can become compromised, leading to an increased permeability, which may result in inflammation and further contribute to neural dysfunction [12]. This may have some implications concerning chronic traumatic encephalopathy, as the hyperphosphorylated tau proteins in CTE can be found not only in the junction between white and grey matter where the shearing of neurons occurs but also around cerebral blood vessels.[13] It is theorized that disruption of the blood-brain barrier, either via stretching and shearing or disruption of the gut-brain axis (discussed further in the next section), may lead to inflammatory or autoimmune responses in the tissue around cerebral blood vessels. This sustained inflammatory response may contribute to the development of CTE or other neurodegenerative diseases. However, more research is needed to draw any definitive conclusions. Furthermore, there is no concrete evidence suggesting that CTE is a direct result of multiple concussion injuries, as studies have demonstrated similar post-mortem findings in the brains of individuals with no history of concussion diagnosis [8].
Inflammatory Changes.
Responding to the insult, resident immune cells in the central nervous system, primarily microglia, become activated. These cells release many inflammatory mediators, including cytokines and chemokines, that permeate brain tissues and potentially contribute to ongoing neuronal damage [9].
Inflammation may persist for days to weeks, causing secondary injury cascades that impair neuronal function and potentiate neurodegeneration. Understanding the breadth and duration of these inflammatory responses remains a current research focus.
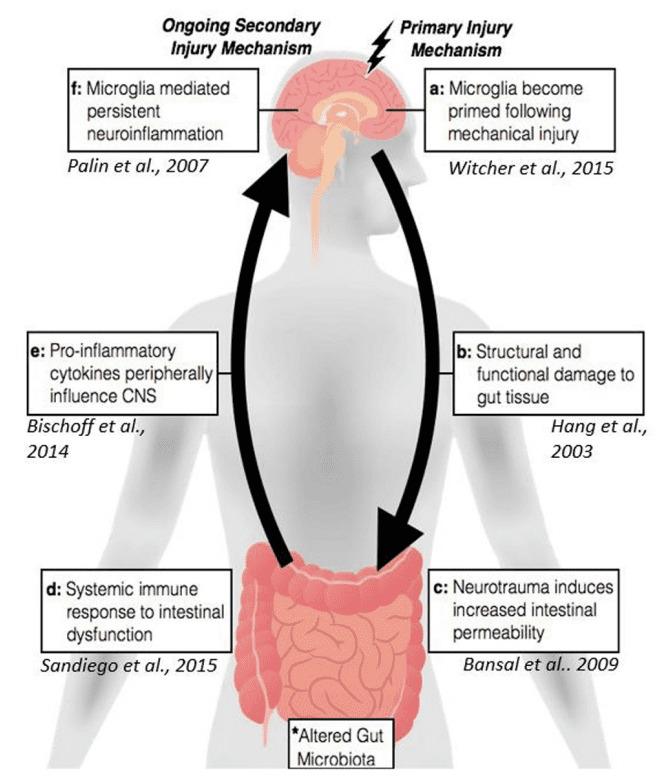
Gut-Brain Connection and Concussion Recovery.
Image from: Sundman MH, Chen NK, Subbian V, Chou YH. The bidirectional gut-brain-microbiota axis as a potential nexus between traumatic brain injury, inflammation, and disease. Brain Behav Immun. 2017 Nov;66:31-44. doi: 10.1016/j.bbi.2017.05.009.
Recent attention has been given to the gut-brain axis in concussion outcomes, acknowledging that brain injuries do not exist in isolation from the rest of the body. The gut microbiome, a complex ecosystem within the gastrointestinal tract, communicates with the central nervous system through multiple pathways — including the vagus nerve, immune system, and various biochemical messengers.
Post-concussion alterations in gut microbiota composition and function can exacerbate neuroinflammation via the gut-brain axis. Dysbiosis — an imbalance in gut microbiome diversity — may influence systemic and central inflammation, impacting recovery trajectories.
Additionally, the bidirectional communication between the gut and the brain suggests that interventions targeting the gut microbiome, such as probiotics, prebiotics, supplementation, or diet modifications, could potentially modulate neuroinflammation and aid in recovery. Understanding the metabolic and inflammatory aftermath of a concussion — and recognizing its interplay with systemic factors like the gut microbiome — is essential for advancing patient care in the field of brain injury.
Conclusion.
Concussion (mTBI) is a mechanical injury with widespread metabolic consequences that kick off with the neurometabolic cascade. This includes ionic flux and a corresponding increase in demand for ATP to restore normal ionic balances. Beyond this, we see alterations in brain blood flow regulation, including changes to cerebrovascular autoregulation, cerebrovascular reactivity, neurovascular coupling, and autonomic control. Additionally, we see the blood-brain barrier (BBB), immune system, and gut microbiome disruption, all of which have pro-inflammatory consequences. Not discussed in this article but also emerging in the literature are hormonal and pituitary changes secondary to mTBI. The pathophysiology of concussion is complex and multi-faceted, and understanding it is essential for clinicians to ensure patients get the appropriate education and treatment for their injury.
References
Giza, C.C. and Hovda, D.A. (2014) ‘The new neurometabolic cascade of concussion’, Neurosurgery, 75(Supplement 4). doi:10.1227/neu.0000000000000505.
Signoretti, S. et al. (2011) ‘The pathophysiology of concussion’, PM&R, 3(10S2). doi:10.1016/j.pmrj.2011.07.018.
R;, H.D. (1999) Improved motor outcome in response to magnesium therapy received up to 24 hours after traumatic diffuse axonal brain injury in rats, Journal of neurosurgery. Available at: https://pubmed.ncbi.nlm.nih.gov/10067920/
Len, T.K. and Neary, J.P. (2010) ‘Cerebrovascular pathophysiology following mild traumatic brain injury’, Clinical Physiology and Functional Imaging [Preprint]. doi:10.1111/j.1475-097x.2010.00990.x.
Wang, Y. et al. (2019) Cerebral blood flow in acute concussion: Preliminary ASL findings from the NCAA-dod care consortium, Brain imaging and behavior. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7232645/
Mutch WA;Ellis MJ;Ryner LN;Graham MR;Dufault B;Gregson B;Hall T;Bunge M;Essig M;Fisher JA;Duffin J;Mikulis DJ; ; ; (2017) Brain Magnetic Resonance Imaging CO2 stress testing in adolescent postconcussion syndrome, Journal of neurosurgery. Available at: https://pubmed.ncbi.nlm.nih.gov/26684777/
Wright AD;Smirl JD;Bryk K;Fraser S;Jakovac M;van Donkelaar P; (2018) Sport-related concussion alters indices of dynamic cerebral autoregulation, Frontiers in neurology. Available at: https://pubmed.ncbi.nlm.nih.gov/29636724/ (Accessed: 14 April 2024).
RJ;, I.G.T.P. (2019) Mild chronic traumatic encephalopathy neuropathology in people with no known participation in contact sports or history of repetitive neurotrauma, Journal of neuropathology and experimental neurology. Available at: https://pubmed.ncbi.nlm.nih.gov/31169877/
Kara N. Corps, D. (2015) Traumatic brain injury, JAMA Neurology. Available at: https://jamanetwork.com/journals/jamaneurology/fullarticle/2091344 (Accessed: 14 April 2024).
Kunces LJ, Keenan J, Schmidt CM, Schmidt MA. Molecular Deficits Relevant to Concussion Are Prevalent in Top-Ranked Football Players Entering the National Football League Draft. J Strength Cond Res. 2021 Nov 1;35(11):3139-3144. doi: 10.1519/JSC.0000000000004131. PMID: 34533486.
May T, Foris LA, Donnally III CJ. Second Impact Syndrome. 2023 Jul 3. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 28846316.
Sahyouni R, Gutierrez P, Gold E, Robertson RT, Cummings BJ. Effects of concussion on the blood-brain barrier in humans and rodents. J Concussion. 2017 Jan-Dec;1:10.1177/2059700216684518. doi: 10.1177/2059700216684518. Epub 2017 Jan 1. PMID: 30828466; PMCID: PMC6391889.
Howell DR, Hunt DL, Aaron SE, Hamner JW, Meehan WP 3rd, Tan CO. Association of Hemodynamic and Cerebrovascular Responses to Exercise With Symptom Severity in Adolescents and Young Adults With Concussion. Neurology. 2021 Nov 30;97(22):e2204-e2212. doi: 10.1212/WNL.0000000000012929. Epub 2021 Oct 11. PMID: 34635563; PMCID: PMC8641971.
Dr. Bradford is a chiropractor and a graduate of the Canadian Memorial Chiropractic College in 2017. He began pursuing additional training in concussion rehabilitation after working with competitive cheerleaders and observing significant gaps in the knowledge delivered in the chiropractic curriculum.
Dr. Bradford now works as part of a multidisciplinary team at Altum Health, with a focus in concussion rehabilitation following workplace injuries and motor vehicle accidents. He also operates a small practice out of his home in Cambridge, Ontario where he grew up.
Dr. Bradford’s approach to patient care includes education, myofascial release, acupuncture, joint manipulation and physical rehabilitation, empowering patients to play an active and informed role in their recovery.