Concussions can happen to athletes of any age participating in all kinds of sports. From hard hits in hockey and football to accidents in gymnastics and soccer, concussions are an…
Greater Toronto Area’s Leading Multidisciplinary Clinics for Concussion Recovery
Concussions are a common form of traumatic brain injury, often caused by blows to the head. They can result in an array of physical, cognitive, and emotional symptoms that may…
Why You Should Never Skip the Neck in Concussion Evaluation & Rehab.
Every patient with a concussion is a patient with a neck injury. Let me explain. A concussion results when the brain undergoes such rapid acceleration-deceleration that shearing and stretching of…
Rethinking Concussion Recovery: The Case for Active Rehabilitation Concussions are more than just a bump on the head, or “getting your bell rung”; they are a type of mild traumatic…
Tinnitus refers to the perception of sound coming from the ear when there are no sources of external sound waves. Tinnitus can be intermittent or constant, in one ear or both ears, and can be caused by a variety of conditions including mild traumatic brain injury.
The sound associated with tinnitus is usually described as a high-pitched ringing in the ears but can vary between individuals.
Some other common descriptions of the sound associated with tinnitus include:
Hissing
Static
Buzzing
Whooshing
Pulsing
Dial tones
Tinnitus is experienced by 10-15% of the adult population at some point in their lives, with 1 in 5 people required medical intervention for their symptoms. After traumatic brain injury, tinnitus is experienced in 53% of cases, with 92% of patients experiencing some form of auditory dysfunction (1). The most common cause of mTBI-related tinnitus is blast injuries such as those experienced by military personal or construction workers.
Common Types of Tinnitus
There are 4 main types of tinnitus: Subjective, sensory, somatic and objective. In each of these types of tinnitus, the root cause and treatment will vary. Therefore, determining the type of tinnitus that a patient is presenting with is an important part of their treatment plan.
Subjective Tinnitus
Subjective tinnitus is the most common form of tinnitus. The symptoms of the tinnitus are only heard by the affected individual and is most commonly caused by exposure to loud noises. Subjective tinnitus episodes usually appear and disappear randomly, and can last between 3-9 months after the symptoms first appear. In severe cases, the symptoms may never fully resolve.
Sensory tinnitus
Sensory tinnitus is caused by a dysfunction in the auditory system itself and is linked to an auditory disorder. A common cause of sensory tinnitus is Meniere’s disease, where fluid build up in the inner ear leads to dysfunction of the labyrinth system, creating symptoms of hearing loss, dizziness and tinnitus.
Somatic tinnitus
Somatic tinnitus is related to movement or proprioception of the head and neck. In somatic tinnitus, symptoms are worsened by specific movements or positions of the affected muscles, joints or other somatic structures that provoke the symptoms of tinnitus.
Objective tinnitus
Objective tinnitus is the rarest type of tinnitus and can be caused by a structural abnormality such as an involuntary muscle contraction or vascular deformities in the auditory system. Once the exact cause of the tinnitus is determined and treated, the symptoms of tinnitus in these patients disappear entirely. It is also the only form of tinnitus where the symptoms can be heard by an outside observer.
Other subtypes of tinnitus
There are also subclassifications of tinnitus that are based on the type of symptoms that the patient is presenting with rather than the cause of the tinnitus. These include musical tinnitus, pulsatile tinnitus, and low frequency tinnitus to name a few of the more common subtypes.
NOTE: If your patient presents with pulsatile tinnitus (tinnitus that increases and decreases with their heart beat), you must refer them for further evaluation as it may be a sign of a life threatening condition such as carotid cavernous fistulas, arteriovenous malformations, and carotid dissections.
How is Tinnitus Diagnosed?
Unfortunately, there is currently no clinical consensus or guideline regarding the diagnosis and treatment of tinnitus caused by head injury. However, this is a growing area of research and there are some general guidelines for how to diagnose it. The diagnostic criteria for tinnitus is:
Ear or head noise that lasts at least 5 minutes and occurs at least twice a week with no source of external sound waves (2).
Tinnitus is usually diagnosed from subjective symptoms alone, but it is important to conduct a thorough history to determine which type of tinnitus the patient is presenting with. This includes when the tinnitus started, what is the character of the tinnitus, things that make it better or worse (head position, ambient noise, activity, etc), their level of hearing loss, how it is affecting their mental state and activities of daily living, any other associated symptoms, previous medical history, etc.
It is also important to rule out “red flag” tinnitus such as those that are pulsatile, are causing severe psychological symptoms, or are associated with other “red flag” symptoms such as new or worsening headache, alterations in sensory or motor function, severe or progressive vestibular symptoms, etc. These patients should be referred for further treatment and investigation into the cause of their tinnitus.
How do you Develop Tinnitus After a Mild Traumatic Brain Injury?
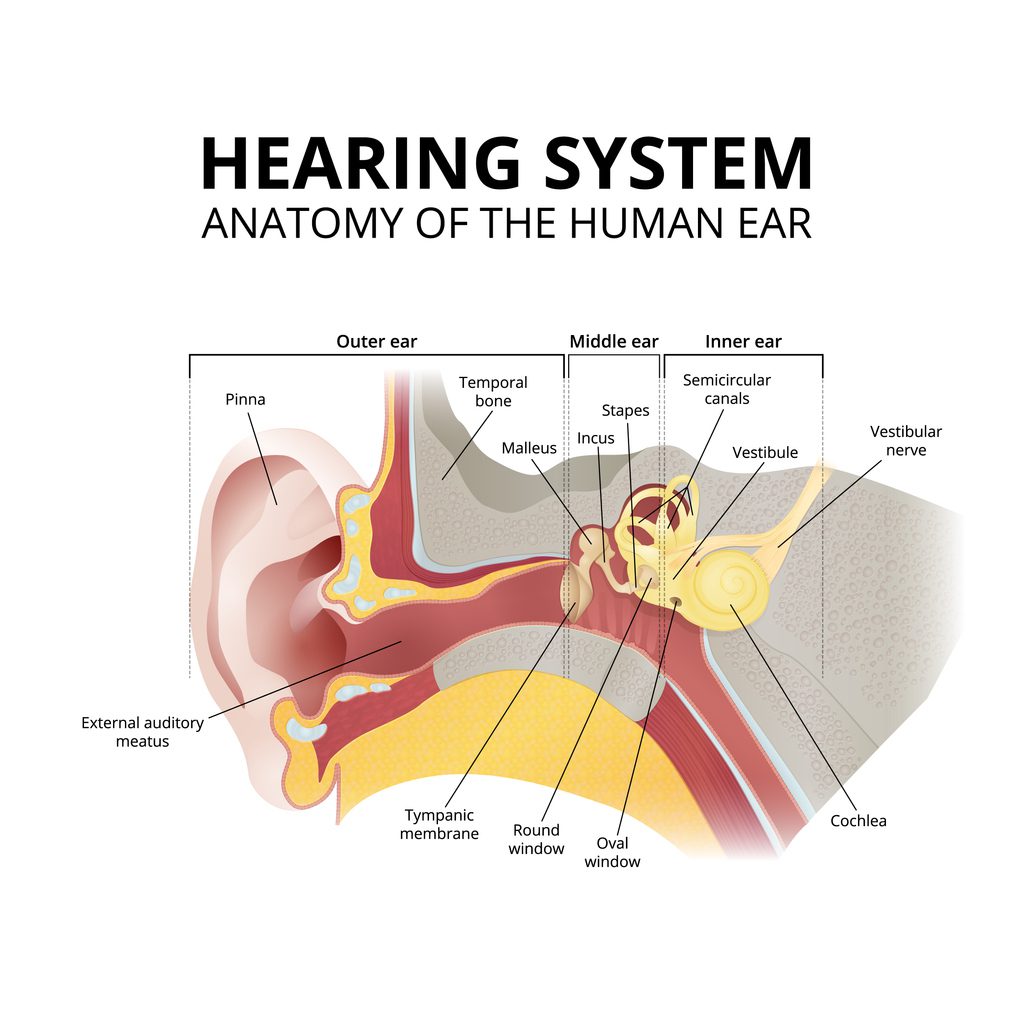
Due to the mechanism of injury of mTBI, the same force that is transmitted through the brain causing brain injury is also transmitted through the middle ear and inner ear which can cause disruption to their function and lead to tinnitus. There are five main causes of tinnitus after head injuries:
Sensorineural Hearing Loss
Sensorineural hearing loss is caused by damage to the inner ear leading to a lack of auditory nerve function. This includes damage to the auditory nerve, rupture of the tympanic membrane, labyrinthine hemorrhage, temporal bone fracture, etc. When the higher-order auditory pathways lose input from the periphery, they enter a hyper-excitable state, which alters the system’s balance between excitation and inhibition. This leads to auditory brain areas receiving auditory signals that did not originate in the periphery, but from other pathway neurons, generating spontaneous “sounds” that are experienced as tinnitus. This hypothesis is similar to that regarding the development of chronic neuropathic pain.
Labyrinthine Concussion
A labyrinthine concussion occurs in the labyrinth of the inner ear and can lead to sensorineural hearing loss, dizziness and tinnitus. While the exact mechanism is not known, it is hypothesized that the acceleration-deceleration injury causes the membranous labyrinth and bony labyrinth to collide, leading to dysfunction of the sensory epithelium. Labyrinthine concussion is usually unilateral, with tinnitus developing immediately or in the hours to days after the injury.
Ossicular Chain Disruption
The ossicular chain is a series of 3 bones in the middle ear: the malleus, incus and stapes. Together, they comprise the primary source of conductive hearing, where these series of bones transmit sound waves from the tympanic membrane to the oval window. After a head injury, there can be alteration or damage to this pathway via the rapid acceleration and deceleration of the head, leading to conductive hearing loss and tinnitus symptoms.
Musculoskeletal Disorders/ Dysfunction
Musculoskeletal conditions can create or worsen tinnitus in patients that have had a head injury. While the exact mechanism is not completely understood, the leading hypothesis is that there is cross activation of the sensory and auditory systems via the dorsal cochlear nucleus (DCN). Muscle and joint dysfunction can activate the somatosensory system, whose signals can cross-activate the DCN in the brainstem, which the auditory system interprets as “sound”. Common musculoskeletal conditions that present with tinnitus include temporomandibular joint dysfunction, sternocleidomastoid strain/ spasm, along with forceful contraction of other head and neck muscles (3).
Psychological Factors
Psychological factors such as anxiety and depression are known risk factors for the development of tinnitus. In division I athletes that have sustained a concussion, 20% experience depression and 33% experience anxiety after their injury. Therefore, it is important to evaluate tinnitus patients for psychological symptoms as it may be involved in both the development and severity of their tinnitus symptoms. (4)
How is Tinnitus Treated?
Referral to an Audiologist or Otologist
Co-managing tinnitus with an audiologist or otologist is an important consideration when treating tinnitus after head injury. Because of the complex and heterogeneous nature of tinnitus, it is recommended that patients are referred to a specialist for further diagnosis, especially if they have chronic tinnitus.
In patients that are experiencing hearing loss in addition to tinnitus, this is especially important as it will expedite the process of them getting prescribed and fitted for a hearing aid which is a key part in helping them manage tinnitus.
Pharmacotherapy
There are several pharmaceutical options that may be prescribed to patients with long-standing tinnitus that have varying levels of efficacy. Currently, the only drugs that outperform placebo in randomized trials are nortriptyline, amitriptyline, alprazolam, clonazepam, and oxazepam.
Other options include injection of lidocaine into muscles that are causing somatic tinnitus. One study saw reductions in tinnitus after lidocaine injections into the lateral pterygoid muscles (5)
Tinnitus Retraining Therapy
Tinnitus retraining therapy (TRT) is a form of habituation therapy that targets the limbic and autonomic nervous systems to reduce the symptoms of tinnitus. TRT attempts to use the plasticity of the brain to train it to become habituated to the sound of the tinnitus and “tune it out”. TRT consists of two main components: sound therapy and retraining counseling (similar to CBT). It aims to change the patient’s emotional perception of tinnitus, and habituate the brain to persistent sound to decrease the conscious experience of the signal. Generally, TRT requires 18 months to achieve observable long term effects and does not work in all patients (6).
Sound Therapy
Sound therapy is based on increasing the background neuronal activity of the auditory system by exposing patients to neutral, low-level, non-intrusive, continuous sounds to help mask the tinnitus and allow them to better focus on activities of daily living. Sounds should not be meaningful, distracting, pleasant or arousing in any way. The sound is played bilaterally and just loud enough that the patient cannot perceive the tinnitus and the sound separately. Sound therapy is particularly helpful for patients who have sleep difficulties due to tinnitus. Examples of sounds include running water, rain, white noise or wind.
Cognitive Behavioral Therapy (CBT)
CBT focuses on retraining how patients think about their symptoms of tinnitus, and focuses on avoiding the negative ideation of the condition. It involves trying to teach patients to replace negative thinking with more positive beliefs. It can also include treatments such as relaxation techniques, acceptance therapy, positive imagery, attention control and others.
Musculoskeletal Rehabilitation
A complete physical rehabilitation program can be an important component of the plan of management for patients with somatic tinnitus where movement of the neck or jaw makes their tinnitus worse. This can include manual therapy to the affected joints/ muscles, muscle stretching and strengthening, and other modalities to improve cervical and temporomandibular joint function.
Hearing Aids
Hearing aids are another treatment option for tinnitus patients that also experience significant hearing loss. By amplifying the intensity of the surrounding external sound waves, the patient can more easily focus on meaningful sounds rather than their tinnitus. A hearing aid can also help to mask the sound generated by tinnitus, decreasing the overall symptom burden.
Conclusion.
In conclusion, tinnitus after traumatic brain injury is a complex but common phenomenon that can have a significant and long lasting impact on patients’ everyday lives. It is important to take the time to correctly diagnose the specific type of tinnitus that the patient is experiencing, and provide the correct plan of management for their specific case. This can include any combination of musculoskeletal rehabilitation, sound therapy, cognitive behavioural therapy, pharmaceutical management, hearing assistive devices, tinnitus retraining therapy and should include referral to an audiologist or otologist if required.
References
Knoll RM, Herman SD, Lubner RJ, et al. Patient-reported auditory handicap measures following mild traumatic brain injury. Laryngoscope. 2020;130(3):761–767.
Dauman R, Tyler RS. Some considerations on the classification of tinnitus. In: Aran J-M, Dauman R, eds. Proceedings of the Fourth International Tinnitus Seminar. Amsterdam/New York: Kugler Publications; 1992:225-229.
Yang J, Peek-Asa C, Covassin T, Torner JC. Post-concussion symptoms of depression and anxiety in division I collegiate athletes. Dev Neuropsychol. 2015 Jan;40(1):18-23. doi: 10.1080/87565641.2014.973499. PMID: 25649775.
Björne A. Assessment of temporomandibular and cervical spine disorders in tinnitus patients. Prog Brain Res. 2007;166:215–219.
Han BI, Lee HW, Kim TY, Lim JS, Shin KS. Tinnitus: characteristics, causes, mechanisms, and treatments. J Clin Neurol. 2009 Mar;5(1):11-9. doi: 10.3988/jcn.2009.5.1.11. Epub 2009 Mar 31. PMID: 19513328; PMCID: PMC2686891.
Dr. Steven Murray is a chiropractor located in downtown Toronto, Canada at Back in Balance clinic with an active living and rehabilitation-based practice. He has a special interest in working with all people of all athletic abilities to reach their fitness and wellness goals. Dr. Murray completed his undergraduate and Master’s degree in Exercise physiology at McGill University. He also completed his Doctor of Chiropractic degree at Canadian Memorial Chiropractic College. Dr. Murray treats a variety of spine related conditions, but also has a special interest in treatment of acute and chronic concussions, along with running- related injuries. In practice, he uses his previous experience in research to provide patients with the most up-to-date evidence-based treatment, so his patients receive a proven treatment plan that is tailored to their specific needs.